Department of Health Systems, Management and Policy, Colorado School of Public Health, University of Colorado, Aurora, CO, USA.
Br J Cancer. 2012 Mar 13;106(6):1100-6. doi: 10.1038/bjc.2012.60. Epub 2012 Feb 28.
New oncology drugs are being developed in conjunction with companion diagnostics with approval restricting their use to certain biomarker-positive subgroups. We examined the impact of different predictive biomarker screening techniques and population enrichment criteria on the cost-effectiveness of targeted drugs in lung cancer, using ALK and crizotinib to build the initial model.
Health economic modeling of cost per Quality Adjusted Life Year was based on literature review and expert opinion. The modeled population represented advanced non-small cell lung cancer (NSCLC), eligible for predictive biomarker screening with prescribing restricted to biomarker-positive patients.
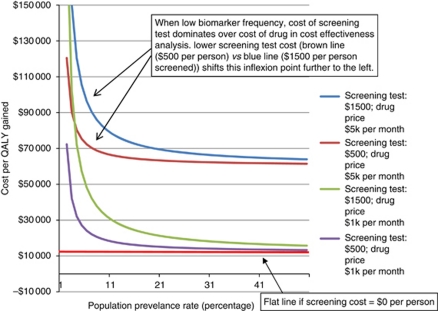
For assays costing $1400 per person, cost per quality-adjusted life year (QALY) gained for ALK screening all advanced NSCLC, excluding treatment cost, is $106,707. This falls to $4756 when only a highly enriched population is screened (increasing biomarker frequency from 1.6 to 35.9%). However, the same enrichment involves missing 56% patients who segregate within the unscreened group. Cheaper screening tests that miss some true positives can be more cost-effective if proportional reductions in cost exceed proportion of subjects missed. Generic modeling of idealised screening assays, including treatment cost, reveals a dominant effect of screening cost per person at low biomarker frequencies. Cost-effectiveness of <$100,000 per QALY gained is not achievable at biomarker frequencies <5% (with drug costs $1-5000 per month and screening costs $600-1400 per person).
Cost-effectiveness of oncology drugs whose prescribing is restricted to biomarker-positive subgroups should address the cost of detecting marker-positive patients. The cost of screening dominates at low frequencies and strategies to improve cost-effectiveness based on the assay cost, drug cost and the group screened should be considered in these scenarios.
新的肿瘤药物与伴随诊断一起开发,批准将其使用限制在某些生物标志物阳性亚组。我们使用 ALK 和克唑替尼构建初始模型,研究了不同预测生物标志物筛选技术和人群富集标准对肺癌靶向药物成本效益的影响。
基于文献回顾和专家意见,对每质量调整生命年的成本进行健康经济学建模。模型人群代表晚期非小细胞肺癌(NSCLC),有资格进行预测生物标志物筛选,仅对生物标志物阳性患者进行处方。
对于每人 1400 美元的检测费用,ALK 筛查所有晚期 NSCLC(不包括治疗费用)的每质量调整生命年(QALY)成本为 106707 美元。当仅对高度富集的人群进行筛选时,这一成本降至 4756 美元(将生物标志物频率从 1.6 增加到 35.9%)。然而,同样的富集方法会错过 56%在未筛选组中分类的患者。如果检测费用的减少比例超过错过的患者比例,那么错过一些真阳性患者的更廉价的筛选测试可能会更具成本效益。包括治疗费用在内的理想化筛选检测的通用模型表明,在低生物标志物频率下,每人的筛选成本对成本效益具有主导作用。在生物标志物频率<5%(药物成本为每月 10000 美元至 5000 美元,每人筛查成本为 600 美元至 1400 美元)的情况下,每获得一个 QALY 的成本效益低于 10 万美元的情况无法实现。
限制在生物标志物阳性亚组使用的肿瘤药物的成本效益应考虑到检测标记阳性患者的成本。在低频率下,筛选成本占主导地位,应考虑基于检测成本、药物成本和筛选人群的策略来提高成本效益。