Fox Chase Cancer Center, Philadelphia, PA 19111, USA.
J Appl Clin Med Phys. 2012 Mar 8;13(2):3708. doi: 10.1120/jacmp.v13i2.3708.
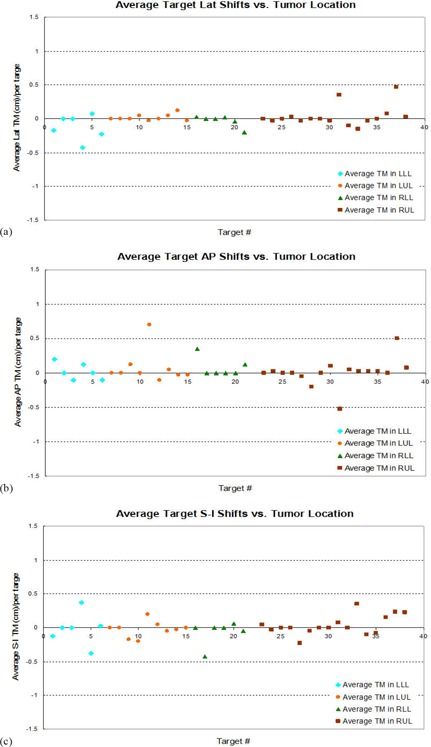
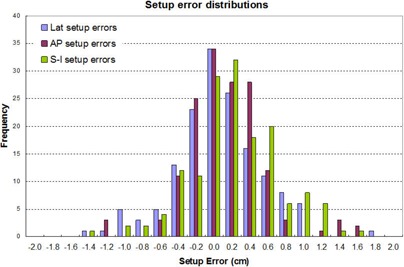
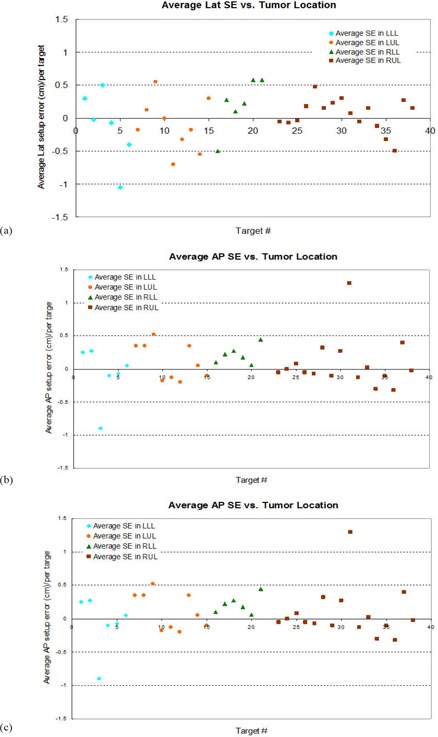
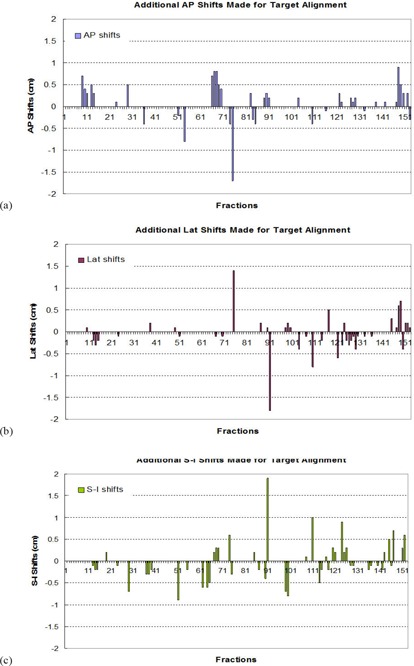
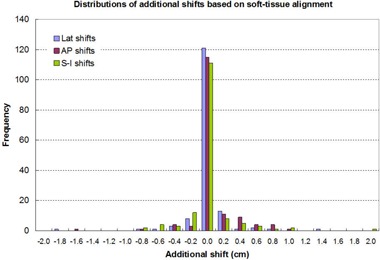
The purpose of this study was to assess target repositional accuracy with respect to the bony structures using daily CBCT, and to validate the planning target volume (PTV) margin used in the lung SBRT. All patients underwent 4D CT scanning in preparation for lung SBRT. The internal target volume (ITV) was outlined from the reconstructed 4D data using the maximum-intensity projection (MIP) algorithm. A 6 mm margin was added to the ITV to create the PTV. Conformal treatment planning was performed on the helical images, to which the MIP images were fused. Prior to each treatment, CBCT was taken after a patient was set up in the treatment position. The CBCT images were fused with the simulation CT based on the bony anatomy, in order to derive setup errors and separate them from the tumor repositional errors. The treating physician then checked and modified the alignment based on target relocalization within the PTV. The shifts determined in such a method were recorded and the subtractions of these shifts with respect to the corresponding setup errors were defined as the target relocalization accuracy. Our study of 36 consecutive patients, treating 38 targets for a total of 153 fractions shows that, after setup error correction, the target repositional accuracy followed a normal distribution with the mean values close to 0 in all directions, and standard deviations of 0.25 cm in A-P, 0.24 cm in Lat, and 0.28 cm in S-I directions, respectively. The probability of having the shifts ? 0.6 cm is less than 0.8% in A-P, 0.6% in Lat, and 1.7 % in S-I directions. For the patient population studied, the target centroid position relative to the bony structures changed minimally from day to day. This demonstrated that the PTV margin that is designed on the MIP image-based ITV was adequate for lung SBRT.
本研究旨在使用每日 CBCT 评估针对骨性结构的靶区重定位准确性,并验证用于肺部 SBRT 的计划靶区(PTV)边界。所有患者在接受肺部 SBRT 治疗前均接受了 4D CT 扫描。使用最大强度投影(MIP)算法从重建的 4D 数据中勾画内部靶区(ITV)。在 ITV 上添加 6mm 边界以创建 PTV。在螺旋 CT 上进行适形治疗计划,并将 MIP 图像融合到该计划中。在每次治疗前,患者在治疗位置设置后进行 CBCT 扫描。根据骨性解剖结构将 CBCT 图像与模拟 CT 融合,以获得设置误差并将其与肿瘤重定位误差分开。然后,主治医生根据 PTV 内的靶区重新定位检查并修改对准。以这种方法确定的移位被记录下来,并且这些移位与相应的设置误差的差值被定义为靶区重定位准确性。我们对 36 例连续患者进行了研究,共治疗了 38 个靶区,总计 153 个分次,结果表明,在进行设置误差校正后,在所有方向上,靶区重定位准确性均接近 0,呈正态分布,均值接近 0,平均值分别为 0.25cm、0.24cm 和 0.28cm。在 A-P、Lat 和 S-I 方向上,移位? 0.6cm 的概率均小于 0.8%、0.6%和 1.7%。对于所研究的患者人群,相对于骨性结构,靶区中心位置每天的变化很小。这表明,基于 MIP 图像 ITV 设计的 PTV 边界对于肺部 SBRT 是足够的。