UZ Brussel, Laboratory of Clinical Chemistry and Radio-immunology, Vrije Universiteit Brussel, Brussel, Belgium.
Hum Reprod. 2012 Jun;27(6):1829-39. doi: 10.1093/humrep/des101. Epub 2012 Apr 3.
This study evaluated the predictive value of serum and follicular fluid (FF) concentrations of anti-Müllerian hormone (AMH) with respect to treatment outcome variables in an IVF cycle.
A retrospective analysis was performed with data from 731 normogonadotrophic women undergoing controlled ovarian stimulation after stimulation with highly purified menotrophin (HP-hMG) or rFSH following a long GnRH agonist protocol.
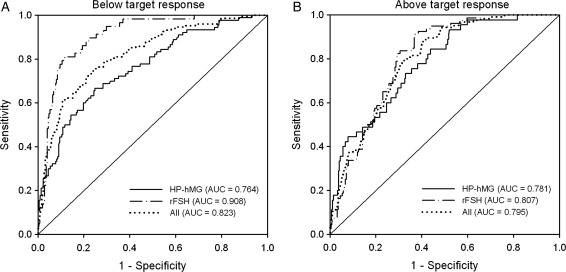
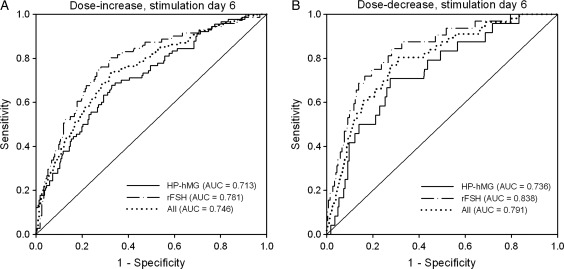
In both treatment groups, the serum AMH concentration at the start of the stimulation was significantly (P < 0.001) positively correlated with the serum levels of estradiol (HP-hMG: r = 0.45; rFSH: r = 0.55), androstenedione (HP-hMG: r = 0.50; rFSH: 0.49) and total testosterone (HP-hMG: r = 0.40; rFSH: r = 0.36) at the end of the stimulation as well as the number of oocytes retrieved (HP-hMG: r = 0.48; rFSH: r = 0.62), the AMH concentration in FF (HP-hMG: r = 0.55; rFSH: 0.61) and the serum progesterone concentration (HP-hMG: r = 0.39; rFSH: r = 0.50) at oocyte retrieval. For both treatments, serum AMH at the start of the stimulation was a good predictor of the need to increase or decrease the gonadotrophin dose on stimulation day 6 and of ovarian response below (<7 oocytes) or above (>15 oocytes) the target. No significant relationships were observed between serum AMH and embryo quality or ongoing pregnancy.
The serum AMH concentration at the start of the stimulation in IVF patients down-regulated with GnRH agonist in the long protocol revealed a positive relationship with ovarian response to gonadotrophins in terms of oocytes retrieved and accompanying endocrine response. AMH is a good predictor of the need for gonadotrophin-dose adjustment on stimulation day 6 for patients with a fixed starting dose, but a poor predictor of embryo quality and pregnancy chances in individual patients.
本研究评估了血清和卵泡液(FF)抗苗勒管激素(AMH)浓度对体外受精(IVF)周期中治疗结局变量的预测价值。
对接受高纯促性腺激素(HP-hMG)或 rFSH 刺激后进行长 GnRH 激动剂方案控制性卵巢刺激的 731 例正常促性腺激素女性患者的数据进行回顾性分析。
在两组治疗中,刺激开始时的血清 AMH 浓度与刺激结束时血清雌二醇(HP-hMG:r = 0.45;rFSH:r = 0.55)、雄烯二酮(HP-hMG:r = 0.50;rFSH:0.49)和总睾酮(HP-hMG:r = 0.40;rFSH:r = 0.36)水平呈显著正相关(P < 0.001),与取卵数(HP-hMG:r = 0.48;rFSH:r = 0.62)、FF 中 AMH 浓度(HP-hMG:r = 0.55;rFSH:0.61)和取卵时血清孕酮浓度(HP-hMG:r = 0.39;rFSH:r = 0.50)呈显著正相关。对于两种治疗方法,刺激开始时的血清 AMH 是预测需要增加或减少刺激第 6 天促性腺激素剂量以及卵巢反应低于(<7 个卵)或高于(>15 个卵)目标的良好指标。血清 AMH 与胚胎质量或持续妊娠之间未见显著相关性。
长 GnRH 激动剂方案下调 IVF 患者刺激开始时的血清 AMH 浓度与获卵数和伴随的内分泌反应方面的卵巢对促性腺激素的反应呈正相关。AMH 是预测刺激第 6 天固定起始剂量患者需要调整促性腺激素剂量的良好指标,但对个别患者的胚胎质量和妊娠机会预测不佳。