Bristol Arthritis & Sports Injury Clinic, St Mary's Hospital, Upper Byron Place, Clifton, Bristol, BS8 1JU, UK.
Knee Surg Sports Traumatol Arthrosc. 2012 Jul;20(7):1227-44. doi: 10.1007/s00167-012-1985-7. Epub 2012 Apr 8.
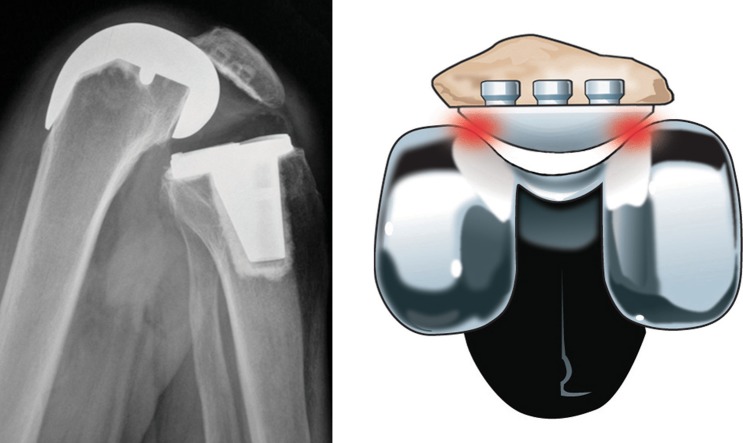
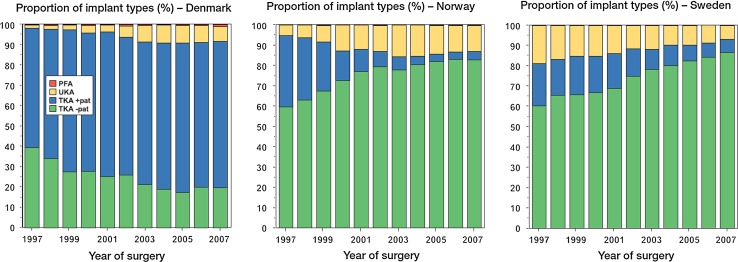
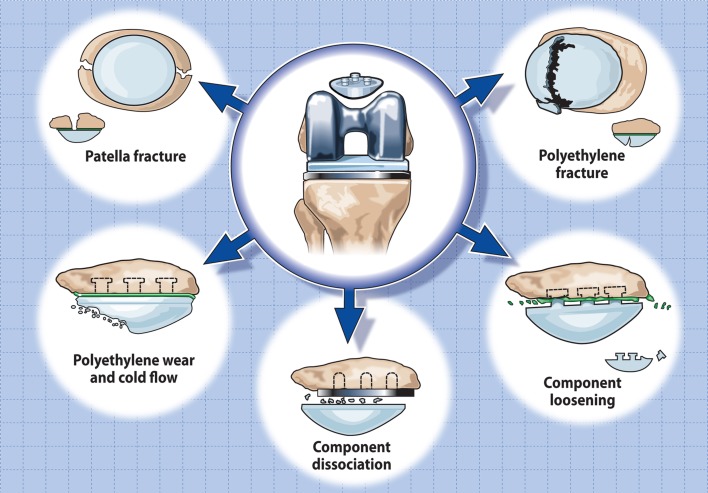
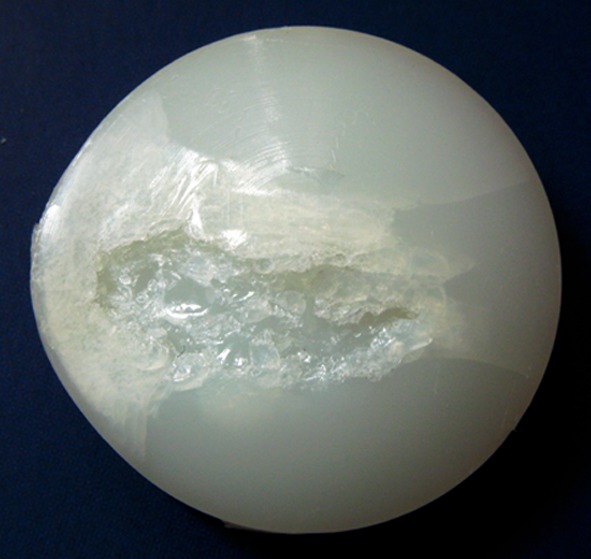
Early arthroplasty designs were associated with a high level of anterior knee pain as they failed to cater for the patello-femoral joint. Patellar resurfacing was heralded as the saviour safeguarding patient satisfaction and success but opinion on its necessity has since deeply divided the scientific community and has become synonymous to topics of religion or politics. Opponents of resurfacing contend that the native patella provides better patellar tracking, improved clinical function, and avoids implant-related complications, whilst proponents argue that patients have less pain, are overall more satisfied, and avert the need for secondary resurfacing. The question remains whether complications associated with patellar resurfacing including those arising from future component revision outweigh the somewhat increased incidence of anterior knee pain recorded in unresurfaced patients. The current scientific literature, which is often affected by methodological limitations and observer bias, remains confusing as it provides evidence in support of both sides of the argument, whilst blinded satisfaction studies comparing resurfaced and non-resurfaced knees generally reveal equivalent results. Even national arthroplasty register data show wide variations in the proportion of patellar resurfacing between countries that cannot be explained by cultural differences alone. Advocates who always resurface or never resurface indiscriminately expose the patella to a random choice. Selective resurfacing offers a compromise by providing a decision algorithm based on a propensity for improved clinical success, whilst avoiding potential complications associated with unnecessary resurfacing. Evidence regarding the validity of selection criteria, however, is missing, and the decision when to resurface is often based on intuitive reasoning. Our lack of understanding why, irrespective of pre-operative symptoms and patellar resurfacing, some patients may suffer pain following TKA and others may not have so far stifled our efforts to make the strategy of selective resurfacing succeed. We should hence devote our efforts in defining predictive criteria and indicators that will enable us to reliably identify those individuals who might benefit from a resurfacing procedure. Level of evidence V.
早期的关节置换设计与高水平的膝关节前痛有关,因为它们不能适应髌股关节。髌骨表面置换被认为是保障患者满意度和成功的救星,但对其必要性的看法自此深深分裂了科学界,并已成为宗教或政治话题的代名词。反对表面置换的人认为,原生髌骨提供更好的髌骨跟踪、改善临床功能,并避免与植入物相关的并发症,而赞成者则认为患者疼痛更少、总体满意度更高,并避免需要二次表面置换。问题仍然是,髌骨表面置换相关的并发症,包括未来组件翻修引起的并发症,是否超过未表面置换患者记录的稍高的膝关节前痛发生率。目前的科学文献,由于方法学限制和观察者偏见,往往令人困惑,因为它提供了支持双方论点的证据,而比较表面置换和非表面置换膝关节的盲法满意度研究通常显示出等效的结果。即使是国家关节置换登记数据,也显示出各国之间髌骨表面置换比例的差异很大,这不能仅用文化差异来解释。不分青红皂白地总是进行表面置换或从不进行表面置换的支持者将髌骨暴露在随机选择中。选择性表面置换提供了一种妥协,通过提供基于临床成功改善倾向的决策算法,同时避免与不必要的表面置换相关的潜在并发症。然而,关于选择标准有效性的证据缺失,并且何时进行表面置换的决定通常基于直观推理。我们缺乏理解为什么,不管术前症状和髌骨表面置换如何,一些患者在 TKA 后可能会感到疼痛,而另一些患者可能不会,这迄今为止阻碍了我们努力使选择性表面置换策略取得成功。我们应该因此努力定义预测标准和指标,使我们能够可靠地识别那些可能从表面置换手术中受益的个体。证据水平 V。