Ko Kiljun, Sung Duk Hyun, Kang Min Jae, Ko Moon Ju, Do Jong Gul, Sunwoo Hyuk, Kwon Tae Gun, Hwang Jung Min, Park Yoonhong
Department of Physical Medicine and Rehabilitation, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul 135-710, Korea.
Ann Rehabil Med. 2011 Dec;35(6):807-15. doi: 10.5535/arm.2011.35.6.807. Epub 2011 Dec 30.
To ascertain the etiology of non-traumatic plexopathy and clarify the clinical, electrophysiological characteristics according to its etiology.
We performed a retrospective analysis of 63 non-traumatic plexopathy patients that had been diagnosed by nerve conduction studies (NCS) and needle electromyography (EMG). Clinical, electrophysiological, imaging findings were obtained from medical records.
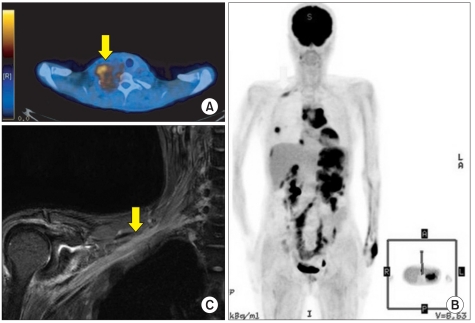
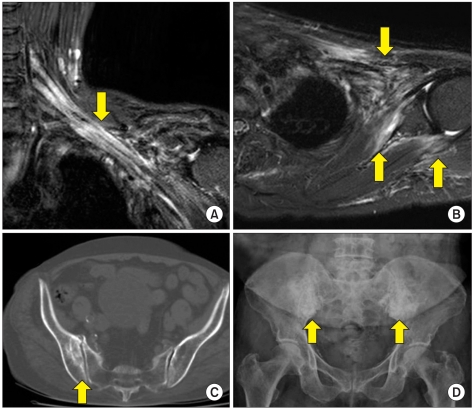
We identified 36 cases with brachial plexopathy (BP) and 27 cases with lumbosacral plexopathy (LSP). The causes of plexopathy were neoplastic (36.1%), thoracic outlet syndrome (TOS) (25.0%), radiation induced (16.7%), neuralgic amyotrophy (8.3%), perioperative (5.6%), unknown (8.3%) in BP, while neoplastic (59.3%), radiation induced (22.2%), neuralgic amyotrophy (7.4%), psoas muscle abscess (3.7%), and unknown (7.4%) in LSP. In neoplastic plexopathy, pain presented as the first symptom in most patients (82.8%), with the lower trunk of the brachial plexus predominantly involved. In radiation induced plexopathy (RIP), pain was a common initial symptom, but the proportion was smaller (50%), and predominant involvements of bilateral lumbosacral plexus and whole trunk of brachial or lumbosacral plexus were characteristic. Myokymic discharges were noted in 41.7% patients with RIP. Abnormal NCS finding in the medial antebrachial cutaneous nerve was the most sensitive to diagnose TOS. Neuralgic amyotrophy of the brachial plexus showed upper trunk involvement in all cases.
By integrating anatomic, pathophysiologic knowledge with detailed clinical assessment and the results of ancillary studies, physicians can make an accurate diagnosis and prognosis.
确定非创伤性臂丛神经病的病因,并根据其病因阐明临床及电生理特征。
我们对63例经神经传导研究(NCS)和针极肌电图(EMG)确诊的非创伤性臂丛神经病患者进行了回顾性分析。从病历中获取临床、电生理及影像学检查结果。
我们识别出36例臂丛神经病(BP)患者和27例腰骶丛神经病(LSP)患者。臂丛神经病的病因包括肿瘤性(36.1%)、胸廓出口综合征(TOS)(25.0%)、放射性损伤(16.7%)、神经性肌萎缩(8.3%)、围手术期(5.6%)、病因不明(8.3%);腰骶丛神经病的病因包括肿瘤性(59.3%)、放射性损伤(22.2%)、神经性肌萎缩(7.4%)、腰大肌脓肿(3.7%)、病因不明(7.4%)。在肿瘤性臂丛神经病中,多数患者(82.8%)以疼痛为首发症状,主要累及臂丛神经下干。在放射性损伤性臂丛神经病(RIP)中,疼痛是常见的初始症状,但比例较小(50%),其特征为双侧腰骶丛神经及臂丛或腰骶丛神经全干受累为主。41.7%的RIP患者出现肌束震颤放电。前臂内侧皮神经NCS异常发现对诊断TOS最敏感。臂丛神经性肌萎缩所有病例均累及上干。
通过将解剖学、病理生理学知识与详细的临床评估及辅助检查结果相结合,医生能够做出准确的诊断和预后判断。