CLAHRC-NDL/Nottingham University Business School, Institute of Mental Health, University of Nottingham Innovation Park, Nottingham, NG7 2TU, UK.
Implement Sci. 2012 May 3;7:40. doi: 10.1186/1748-5908-7-40.
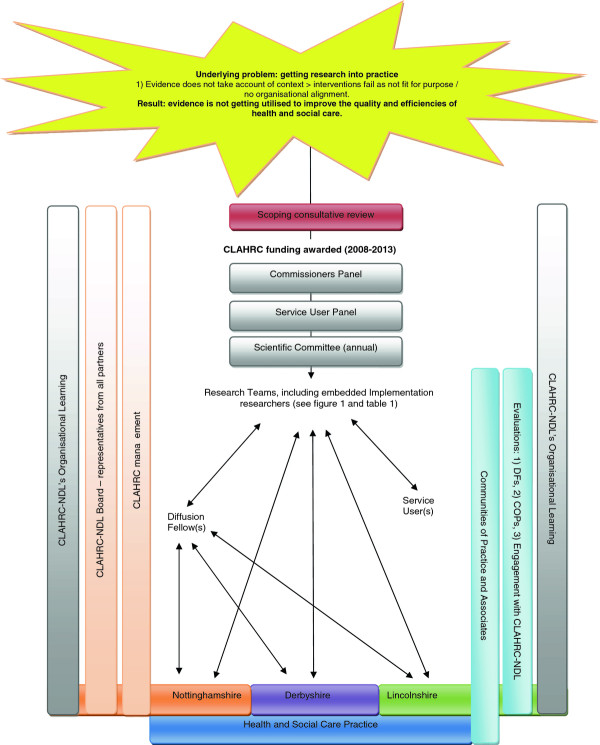
To address the problem of translation from research-based evidence to routine healthcare practice, the Collaboration for Leadership in Applied Health Research and Care for Nottinghamshire, Derbyshire, and Lincolnshire (CLAHRC-NDL) was funded by the National Institute for Health Research as one of nine CLAHRCs across England. This paper outlines the underlying theory and its application that CLAHRC-NDL has adopted, as a case example that might be generalised to practice outside the CLAHRC, in comparison to alternative models of implementation.
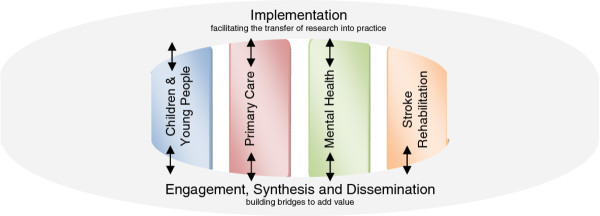
Conventional approaches to health research frequently generate evidence in isolation from the environment in which it is intended for use. The premise of the CLAHRC-NDL model is that barriers to implementation can be overcome if knowledge is co-produced by academic and clinical service staff, taking account of the organisational context in which it is to be applied. This approach is founded on organisational learning theory, recognising that change is a social and political phenomenon. Evidence is produced in real time, taking full account of the environment in which it is to be implemented. To support this process, senior health service staff are seconded to the CLAHRC as 'diffusion fellows' (DFs) to actively bridge the research to practice gap by being a full member of both the research team and their area of clinical practice. To facilitate innovation and embed change in the local health community, existing communities of practice are enhanced and new ones are fostered around specific themes. Our approach has been adopted by 16 clinical research studies in the areas of mental health, children and young people, primary care, and stroke rehabilitation.
The CLAHRC-NDL model of implementation applies organisational learning theory by addressing the social and situational barriers and enablers to implementation, and adopting a philosophy of co-production. Two key mechanisms for translation of innovation have been utilised: DFs, to actively bridge the research to practice gap, and communities of practice, to underpin and sustain improvements in healthcare. The model shows promising results in putting research into practice, which may be transferable to other healthcare contexts.
为了解决将基于研究的证据转化为常规医疗保健实践的问题,诺丁汉、德比和林肯郡应用卫生研究与保健合作组织(CLAHRC-NDL)由英国国家健康研究所资助,作为英格兰九个 CLAHRC 之一。本文概述了 CLAHRC-NDL 采用的基础理论及其应用,作为一个案例研究,可以推广到 CLAHRC 之外的实践中,与替代实施模型进行比较。
传统的健康研究方法经常在与预期使用环境隔离的情况下生成证据。CLAHRC-NDL 模型的前提是,如果学术和临床服务人员共同生产知识,并考虑到其应用的组织背景,可以克服实施障碍。这种方法基于组织学习理论,认识到变革是一种社会和政治现象。证据是实时生成的,充分考虑了其实施的环境。为了支持这一过程,高级卫生服务人员作为“传播研究员”(DF)借调到 CLAHRC,作为研究团队和他们的临床实践领域的正式成员,积极弥合研究与实践之间的差距。为了促进创新并在当地卫生社区中嵌入变革,围绕特定主题增强和培育现有的实践社区。我们的方法已被 16 项心理健康、儿童和青少年、初级保健和中风康复领域的临床研究采用。
CLAHRC-NDL 的实施模型通过解决实施的社会和情境障碍和促进因素,并采用共同生产的理念,应用组织学习理论。已经利用了两种创新转化的关键机制:DF,积极弥合研究与实践之间的差距,以及实践社区,为医疗保健的改进提供支持和维持。该模型在将研究转化为实践方面显示出有希望的结果,可能适用于其他医疗保健环境。