Department of Melanoma, Istituto Nazionale Tumori Fondazione G, Pascale, Naples, Italy.
J Transl Med. 2012 Jul 9;10:85. doi: 10.1186/1479-5876-10-85.
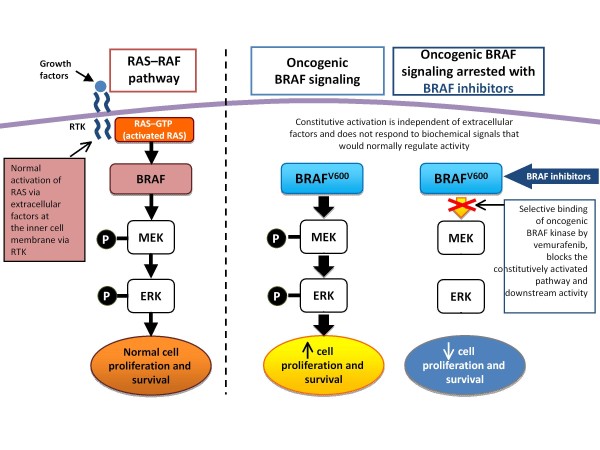
BRAF is a serine/threonine protein kinase activating the MAP kinase/ERK-signaling pathway. About 50 % of melanomas harbors activating BRAF mutations (over 90 % V600E). BRAFV600E has been implicated in different mechanisms underlying melanomagenesis, most of which due to the deregulated activation of the downstream MEK/ERK effectors. The first selective inhibitor of mutant BRAF, vemurafenib, after highly encouraging results of the phase I and II trial, was compared to dacarbazine in a phase III trial in treatment-naïve patients (BRIM-3). The study results showed a relative reduction of 63 % in risk of death and 74 % in risk of tumor progression. Considering all trials so far completed, median overall survival reached approximately 16 months for vemurafenib compared to less than 10 months for dacarbazine treatment. Vemurafenib has been extensively tested on melanoma patients expressing the BRAFV600E mutated form; it has been demonstrated to be also effective in inhibiting melanomas carrying the V600K mutation. In 2011, both FDA and EMA therefore approved vemurafenib for metastatic melanoma carrying BRAFV600 mutations. Some findings suggest that continuation of vemurafenib treatment is potentially beneficial after local therapy in a subset of patients with disease progression (PD). Among who continued vemurafenib >30 days after local therapy of PD lesion(s), a median overall survival was not reached, with a median follow-up of 15.5 months from initiation of BRAF inhibitor therapy. For patients who did not continue treatment, median overall survival from the time of disease progression was 1.4 months. A clinical phase I/II trial is evaluating the safety, tolerability and efficacy of vemurafenib in combination with the CTLA-4 inhibitor mAb ipilimumab. In the BRIM-7 trial vemurafenib is tested in association with GDC-0973, a potent and highly selective inhibitor of MEK1/2. Preliminary data seem to indicate that an additional inhibitor of mutated BRAF, GSK2118436, might be also active on a wider range of BRAF mutations (V600E-K-D-R); actually, treatment with such a compound is under evaluation in a phase III study among stage III-IV melanoma patients positive for BRAF mutations. Overall, BRAF inhibitors were well tolerated; common adverse events are arthralgia, rash, fatigue, alopecia, keratoacanthoma or cutaneous squamous-cell carcinoma, photosensitivity, nausea, and diarrhea, with some variants between different inhibitors.
BRAF 是一种丝氨酸/苏氨酸蛋白激酶,可激活 MAP 激酶/ERK 信号通路。约 50%的黑色素瘤存在激活的 BRAF 突变(超过 90%为 V600E)。BRAFV600E 参与了黑色素瘤发生的多种机制,其中大多数机制归因于下游 MEK/ERK 效应物的失调激活。第一种选择性突变 BRAF 抑制剂 vemurafenib,在 I 期和 II 期试验中取得了令人鼓舞的结果后,与 dacarbazine 进行了 III 期试验,用于治疗初治患者(BRIM-3)。研究结果表明,死亡风险降低了 63%,肿瘤进展风险降低了 74%。考虑到迄今为止完成的所有试验,vemurafenib 的中位总生存期约为 16 个月,而 dacarbazine 治疗的中位总生存期不到 10 个月。vemurafenib 已在表达 BRAFV600E 突变形式的黑色素瘤患者中进行了广泛测试;它还被证明对携带 V600K 突变的黑色素瘤有效。因此,2011 年,FDA 和 EMA 均批准 vemurafenib 用于携带 BRAFV600 突变的转移性黑色素瘤。一些研究结果表明,在疾病进展(PD)的亚组患者中,局部治疗后继续使用 vemurafenib 治疗可能是有益的。在 PD 病变局部治疗后继续使用 vemurafenib >30 天的患者中,中位总生存期未达到,BRAF 抑制剂治疗开始后的中位随访时间为 15.5 个月。对于未继续治疗的患者,从疾病进展时的中位总生存期为 1.4 个月。一项 I/II 期临床试验正在评估 vemurafenib 联合 CTLA-4 抑制剂 mAb ipilimumab 的安全性、耐受性和疗效。在 BRIM-7 试验中,vemurafenib 与 GDC-0973 联合测试,GDC-0973 是一种有效的、高度选择性的 MEK1/2 抑制剂。初步数据似乎表明,另一种突变型 BRAF 抑制剂 GSK2118436 可能对更广泛范围的 BRAF 突变(V600E-K-D-R)也具有活性;实际上,这种化合物的治疗正在 IIIB-IV 期黑色素瘤患者中进行 III 期研究,这些患者的 BRAF 突变呈阳性。总体而言,BRAF 抑制剂具有良好的耐受性;常见的不良反应包括关节痛、皮疹、疲劳、脱发、角化棘皮瘤或皮肤鳞状细胞癌、光敏性、恶心和腹泻,不同抑制剂之间存在一些差异。