Division of Endocrine Surgery, Department of Surgery, The University of Hong Kong, Hong Kong SAR, China.
Ann Surg Oncol. 2012 Oct;19(11):3472-8. doi: 10.1245/s10434-012-2385-4. Epub 2012 May 8.
The prognostic significance of size of central lymph node metastasis (CLNM) in papillary thyroid carcinoma (PTC) remains unknown. Because postsurgical detectable stimulated thyroglobulin (DsTg) after radioiodine ablation may imply persistent or recurrent disease, we evaluated the association between size of CLNM and rate of DsTg in patients with PTC who underwent unilateral prophylactic central neck dissection.
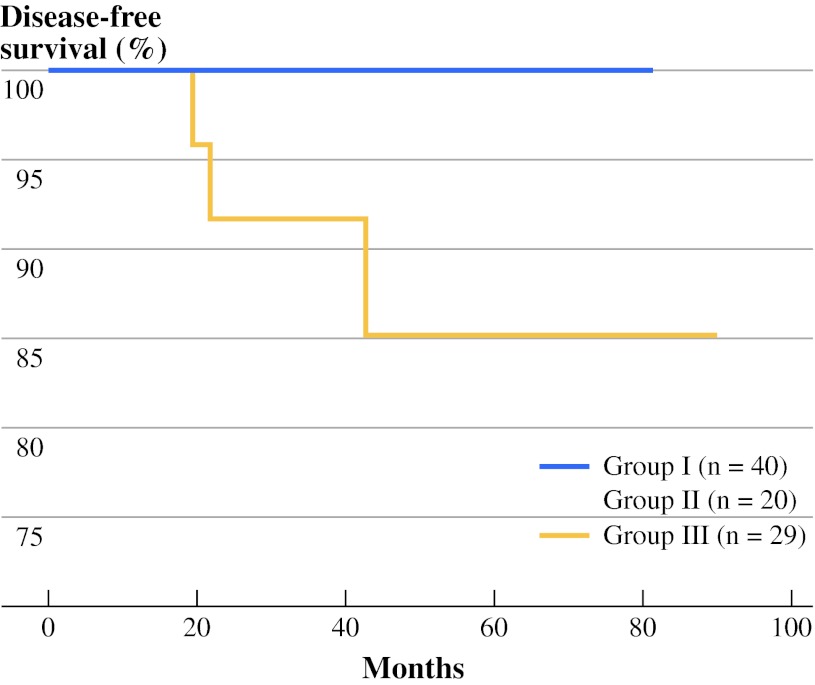
To be eligible for analysis, the prophylactic central neck dissection specimen with <3 central lymph nodes (CLNs) or size of CLNM ≥1 cm as measured under the microscope was excluded. Of 132 specimens, 89 (67.4%) were eligible. Forty patients (44.9%) had no metastasis or pN0, 20 (22.5%) had micrometastasis (<2 mm) or pN1mic and 29 (32.6%) had macrometastasis (≥2 mm) or pN1mac. Postablation sTg level was measured 9 months after surgery. A multivariable analysis was conducted to identify independent factors for postablation DsTg.
Larger-sized CLNM correlated significantly with younger age (p = 0.028), greater number of CLN retrieved (p = 0.016), greater number of metastatic CLN excised (p < 0.001), higher metastatic CLN ratio (p = 0.006) and postablation sTg level (p = 0.012). In the multivariable analysis, after adjusting for tumor size and metastatic CLN ratio, size of CLNM was an independent predictor of postablation DsTg (odds ratio 1.56, 95% confidence interval 1.09-2.24, p = 0.015). Relative to pN0, the odds ratios for postablation DsTg in pN1mic and pN1mac were 2.53 (95% confidence interval 0.35-19.00, p = 0.351) and 5.81 (95% confidence interval 1.22-27.70, p = 0.027), respectively.
Size of CLNM was an independent factor for DsTg 9 months after surgery. Patients with pN1mac were almost 6 times more likely to have postablation DsTg than those with pN0 or pN1mic.
中央区淋巴结转移(CLNM)大小在甲状腺乳头状癌(PTC)中的预后意义尚不清楚。由于放射性碘消融后术后可检测到的刺激甲状腺球蛋白(DsTg)可能意味着持续性或复发性疾病,因此我们评估了行单侧预防性中央区颈部清扫术的 PTC 患者 CLNM 大小与 DsTg 率之间的关系。
为了进行分析,排除预防性中央区颈部清扫术标本中中央淋巴结(CLN)<3 个或显微镜下测量的 CLNM 大小≥1cm 的患者。共 132 例标本中,89 例(67.4%)符合条件。40 例(44.9%)患者无转移或 pN0,20 例(22.5%)患者有微转移(<2mm)或 pN1mic,29 例(32.6%)患者有大转移(≥2mm)或 pN1mac。术后 9 个月测量消融后 sTg 水平。进行多变量分析以确定消融后 DsTg 的独立因素。
较大的 CLNM 与较年轻的年龄(p=0.028)、更多的 CLN 检出(p=0.016)、更多的转移性 CLN 切除(p<0.001)、更高的转移性 CLN 比例(p=0.006)和消融后 sTg 水平(p=0.012)显著相关。在多变量分析中,在调整肿瘤大小和转移性 CLN 比例后,CLNM 大小是消融后 DsTg 的独立预测因素(优势比 1.56,95%置信区间 1.09-2.24,p=0.015)。与 pN0 相比,pN1mic 和 pN1mac 患者消融后 DsTg 的优势比分别为 2.53(95%置信区间 0.35-19.00,p=0.351)和 5.81(95%置信区间 1.22-27.70,p=0.027)。
CLNM 大小是术后 9 个月 DsTg 的独立因素。与 pN0 或 pN1mic 相比,pN1mac 患者消融后 DsTg 的可能性几乎增加 6 倍。