Department of Psychiatry, University of East Anglia, Norwich, United Kingdom.
PLoS One. 2012;7(5):e35185. doi: 10.1371/journal.pone.0035185. Epub 2012 May 2.
Agitation in Alzheimer's disease (AD) is common and associated with poor patient life-quality and carer distress. The best evidence-based pharmacological treatments are antipsychotics which have limited benefits with increased morbidity and mortality. There are no memantine trials in clinically significant agitation but post-hoc analyses in other populations found reduced agitation. We tested the primary hypothesis, memantine is superior to placebo for clinically significant agitation, in patients with moderate-to-severe AD.
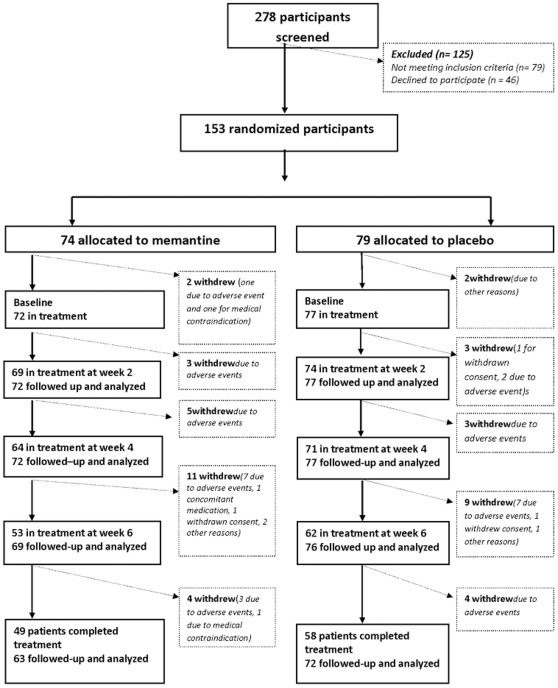
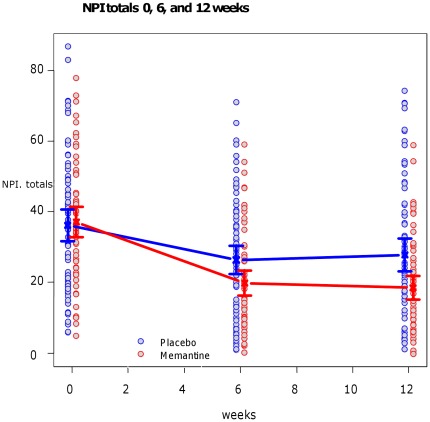
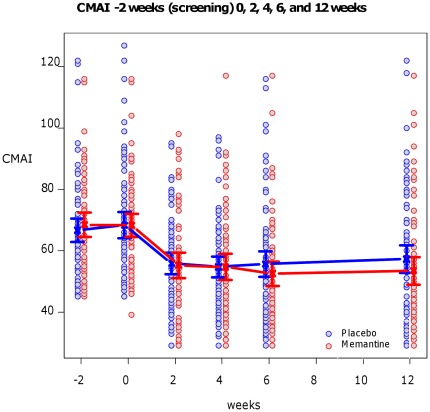
We recruited 153 participants with AD and clinically significant agitation from care-homes or hospitals for a double-blind randomised-controlled trial and 149 people started the trial of memantine versus placebo. The primary outcome was 6 weeks mixed model autoregressive analysis of Cohen-Mansfield Agitation Inventory (CMAI). Secondary outcomes were: 12 weeks CMAI; 6 and 12 weeks Neuropsychiatric symptoms (NPI), Clinical Global Impression Change (CGI-C), Standardised Mini Mental State Examination, Severe Impairment Battery. Using a mixed effects model we found no significant differences in the primary outcome, 6 weeks CMAI, between memantine and placebo (memantine lower -3.0; -8.3 to 2.2, p = 0.26); or 12 weeks CMAI; or CGI-C or adverse events at 6 or 12 weeks. NPI mean difference favoured memantine at weeks 6 (-6.9; -12.2 to -1.6; p = 0.012) and 12 (-9.6; -15.0 to -4.3 p = 0.0005). Memantine was significantly better than placebo for cognition. The main study limitation is that it still remains to be determined whether memantine has a role in milder agitation in AD.
Memantine did not improve significant agitation in people with in moderate-to-severe AD. Future studies are urgently needed to test other pharmacological candidates in this group and memantine for neuropsychiatric symptoms.
ClinicalTrials.gov NCT00371059.
International Standard Randomised Controlled Trial 24953404.
阿尔茨海默病(AD)患者常出现激越,这与较差的患者生活质量和照料者痛苦相关。最好的循证医学治疗药物是抗精神病药,但会增加发病率和死亡率,获益有限。对于有临床意义的激越,美金刚没有临床试验,但其他人群的事后分析发现激越减少。我们测试了主要假设,即美金刚对于中重度 AD 患者有临床意义的激越优于安慰剂。
我们从养老院或医院招募了 153 名 AD 合并有临床意义激越的患者,进行双盲随机对照试验,其中 149 人开始接受美金刚或安慰剂治疗。主要结局是 6 周混合模型自回归分析 Cohen-Mansfield 激越量表(CMAI)。次要结局包括:12 周 CMAI;6 周和 12 周神经精神症状(NPI),临床总体印象变化(CGI-C),标准化简易精神状态检查,严重损伤量表。采用混合效应模型,我们发现美金刚与安慰剂在主要结局(6 周 CMAI)、次要结局(12 周 CMAI,CGI-C)或 6 周和 12 周 NPI 或不良反应方面无显著差异。6 周和 12 周 NPI 均值差值均有利于美金刚(6 周时差值-6.9;-12.2 至-2.2,p=0.26;12 周时差值-9.6;-15.0 至-4.3,p=0.0005)。在认知方面,美金刚显著优于安慰剂。本研究的主要局限性在于仍需确定美金刚在 AD 轻度激越患者中的作用。
美金刚并不能改善中重度 AD 患者的明显激越。急需开展进一步研究,以检验该人群中其他药理学候选药物和美金刚对神经精神症状的作用。
ClinicalTrials.gov NCT00371059。
国际标准随机对照试验 24953404。