Exeter University Medical School, Exeter University, Exeter, United Kingdom.
Institute of Mental Health, University of Nottingham, Nottingham, United Kingdom.
PLoS Med. 2018 Feb 6;15(2):e1002500. doi: 10.1371/journal.pmed.1002500. eCollection 2018 Feb.
Agitation is a common, challenging symptom affecting large numbers of people with dementia and impacting on quality of life (QoL). There is an urgent need for evidence-based, cost-effective psychosocial interventions to improve these outcomes, particularly in the absence of safe, effective pharmacological therapies. This study aimed to evaluate the efficacy of a person-centred care and psychosocial intervention incorporating an antipsychotic review, WHELD, on QoL, agitation, and antipsychotic use in people with dementia living in nursing homes, and to determine its cost.
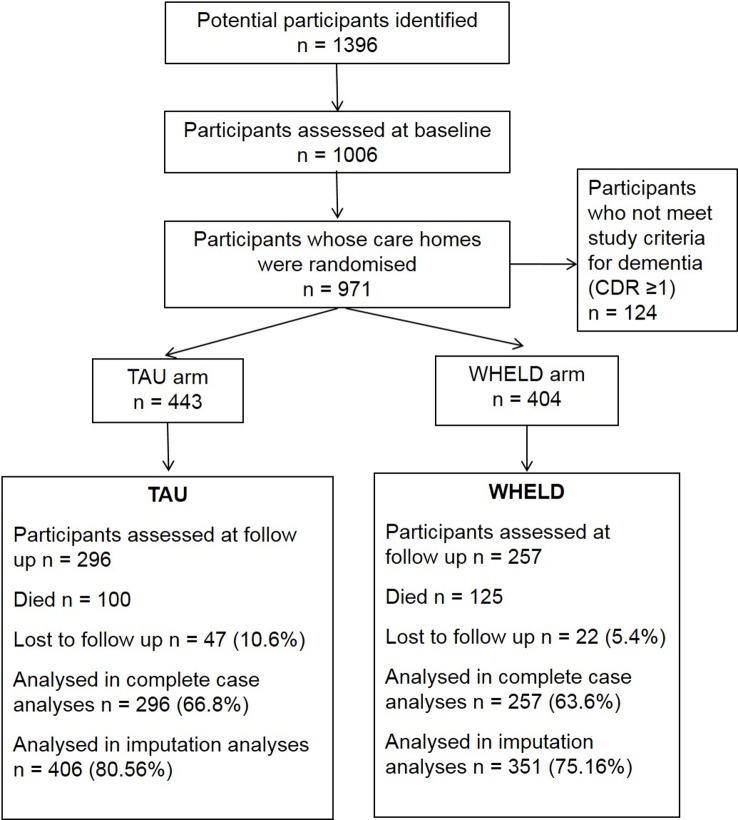
This was a randomised controlled cluster trial conducted between 1 January 2013 and 30 September 2015 that compared the WHELD intervention with treatment as usual (TAU) in people with dementia living in 69 UK nursing homes, using an intention to treat analysis. All nursing homes allocated to the intervention received staff training in person-centred care and social interaction and education regarding antipsychotic medications (antipsychotic review), followed by ongoing delivery through a care staff champion model. The primary outcome measure was QoL (DEMQOL-Proxy). Secondary outcomes were agitation (Cohen-Mansfield Agitation Inventory [CMAI]), neuropsychiatric symptoms (Neuropsychiatric Inventory-Nursing Home Version [NPI-NH]), antipsychotic use, global deterioration (Clinical Dementia Rating), mood (Cornell Scale for Depression in Dementia), unmet needs (Camberwell Assessment of Need for the Elderly), mortality, quality of interactions (Quality of Interactions Scale [QUIS]), pain (Abbey Pain Scale), and cost. Costs were calculated using cost function figures compared with usual costs. In all, 847 people were randomised to WHELD or TAU, of whom 553 completed the 9-month randomised controlled trial. The intervention conferred a statistically significant improvement in QoL (DEMQOL-Proxy Z score 2.82, p = 0.0042; mean difference 2.54, SEM 0.88; 95% CI 0.81, 4.28; Cohen's D effect size 0.24). There were also statistically significant benefits in agitation (CMAI Z score 2.68, p = 0.0076; mean difference 4.27, SEM 1.59; 95% CI -7.39, -1.15; Cohen's D 0.23) and overall neuropsychiatric symptoms (NPI-NH Z score 3.52, p < 0.001; mean difference 4.55, SEM 1.28; 95% CI -7.07,-2.02; Cohen's D 0.30). Benefits were greatest in people with moderately severe dementia. There was a statistically significant benefit in positive care interactions as measured by QUIS (19.7% increase, SEM 8.94; 95% CI 2.12, 37.16, p = 0.03; Cohen's D 0.55). There were no statistically significant differences between WHELD and TAU for the other outcomes. A sensitivity analysis using a pre-specified imputation model confirmed statistically significant benefits in DEMQOL-Proxy, CMAI, and NPI-NH outcomes with the WHELD intervention. Antipsychotic drug use was at a low stable level in both treatment groups, and the intervention did not reduce use. The WHELD intervention reduced cost compared to TAU, and the benefits achieved were therefore associated with a cost saving. The main limitation was that antipsychotic review was based on augmenting processes within care homes to trigger medical review and did not in this study involve proactive primary care education. An additional limitation was the inherent challenge of assessing QoL in this patient group.
These findings suggest that the WHELD intervention confers benefits in terms of QoL, agitation, and neuropsychiatric symptoms, albeit with relatively small effect sizes, as well as cost saving in a model that can readily be implemented in nursing homes. Future work should consider how to facilitate sustainability of the intervention in this setting.
ISRCTN Registry ISRCTN62237498.
激越是一种常见且具有挑战性的症状,影响着大量痴呆患者,影响其生活质量(QoL)。迫切需要基于证据、具有成本效益的心理社会干预措施来改善这些结果,尤其是在缺乏安全有效的药物治疗的情况下。本研究旨在评估以人为中心的护理和心理社会干预措施(包括抗精神病药物审查)对居住在养老院的痴呆患者的 QoL、激越和抗精神病药物使用的疗效,并确定其成本。
这是一项于 2013 年 1 月 1 日至 2015 年 9 月 30 日进行的随机对照集群试验,比较了 WHELD 干预与常规治疗(TAU)在 69 家英国养老院中痴呆患者的效果,采用意向治疗分析。所有分配到干预组的养老院都接受了关于以人为中心的护理和社会互动以及抗精神病药物(抗精神病药物审查)教育的工作人员培训,随后通过护理人员冠军模式进行持续交付。主要结局指标是生活质量(DEMQOL-Proxy)。次要结局指标是激越(Cohen-Mansfield 激越量表[CMAI])、神经精神症状(神经精神疾病护理院版[NPI-NH])、抗精神病药物使用、总体恶化(临床痴呆评定)、情绪(康奈尔抑郁痴呆量表[CDD])、未满足的需求(老年评估需求量表[CAMBERWELL])、死亡率、互动质量(互动质量量表[QUIS])、疼痛(Abbey 疼痛量表)和成本。使用与常规成本相比的成本函数图计算成本。共有 847 人被随机分配到 WHELD 或 TAU 组,其中 553 人完成了为期 9 个月的随机对照试验。该干预措施在生活质量(DEMQOL-Proxy Z 评分 2.82,p = 0.0042;平均差异 2.54,SEM 0.88;95%CI 0.81,4.28;Cohen's D 效应大小 0.24)方面有统计学显著改善。在激越(CMAI Z 评分 2.68,p = 0.0076;平均差异 4.27,SEM 1.59;95%CI -7.39,-1.15;Cohen's D 0.23)和整体神经精神症状(NPI-NH Z 评分 3.52,p < 0.001;平均差异 4.55,SEM 1.28;95%CI -7.07,-2.02;Cohen's D 0.30)方面也有统计学显著的益处。在中度至重度痴呆患者中,益处最大。QUIS(积极护理互动量表)测量的积极护理互动有统计学显著增加(增加 19.7%,SEM 8.94;95%CI 2.12,37.16,p = 0.03;Cohen's D 0.55)。在其他结局方面,WHELD 和 TAU 之间没有统计学显著差异。使用预指定的插补模型进行的敏感性分析证实,WHELD 干预在 DEMQOL-Proxy、CMAI 和 NPI-NH 结局方面具有统计学显著益处。抗精神病药物的使用在两组治疗中都处于低稳定水平,且干预并未减少其使用。与 TAU 相比,WHELD 干预降低了成本,因此所取得的益处与成本节约相关。主要限制因素是抗精神病药物审查是基于增强养老院中的医疗审查过程,而在本研究中并未涉及主动初级保健教育。另一个限制因素是评估这一患者群体生活质量的固有挑战。
这些发现表明,WHELD 干预在 QoL、激越和神经精神症状方面有获益,尽管效果相对较小,同时还可以节省成本,且这种模式很容易在养老院中实施。未来的工作应考虑如何在这种环境下促进干预的可持续性。
ISRCTN 注册 ISRCTN62237498。