Vanderheyden Simon, Casaer Michael P, Kesteloot Katrien, Simoens Steven, De Rijdt Thomas, Peers Guido, Wouters Pieter J, Coenegrachts Jocelijn, Grieten Tine, Polders Katleen, Maes Ann, Wilmer Alexander, Dubois Jasperina, Van den Berghe Greet, Mesotten Dieter
Crit Care. 2012 May 25;16(3):R96. doi: 10.1186/cc11361.
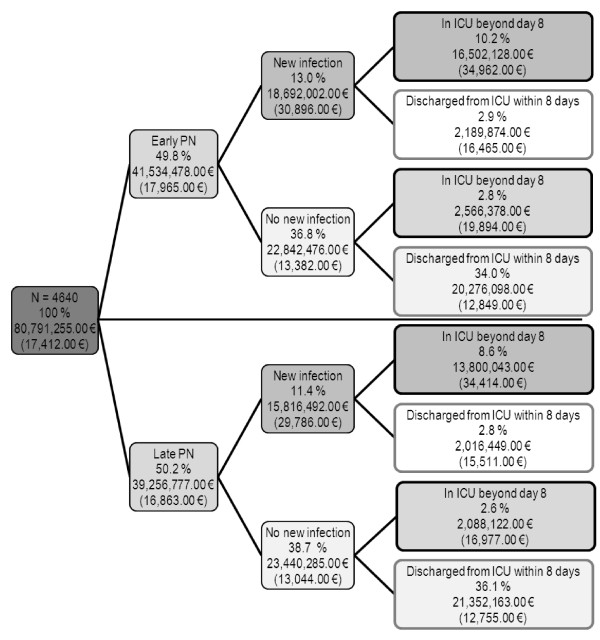
The EPaNIC randomized controlled multicentre trial showed that postponing initiation of parenteral nutrition (PN) in ICU-patients to beyond the first week (Late-PN) enhanced recovery, as compared with Early-PN. This was mediated by fewer infections, accelerated recovery from organ failure and reduced duration of hospitalization. Now, the trial's preplanned cost analysis (N = 4640) from the Belgian healthcare payers' perspective is reported.
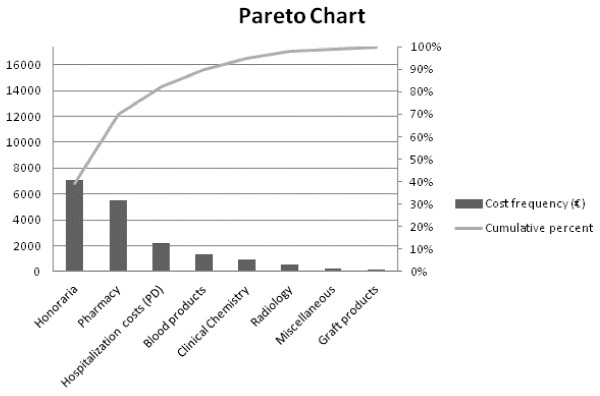
Cost data were retrieved from individual patient invoices. Undiscounted total healthcare costs were calculated for the index hospital stay. A cost tree based on acquisition of new infections and on prolonged length-of-stay was constructed. Contribution of 8 cost categories to total hospitalization costs was analyzed. The origin of drug costs was clarified in detail through the Anatomical Therapeutic Chemical (ATC) classification system. The potential impact of Early-PN on total hospitalization costs in other healthcare systems was explored in a sensitivity analysis.
ICU-patients developing new infection (24.4%) were responsible for 42.7% of total costs, while ICU-patients staying beyond one week (24.3%) accounted for 43.3% of total costs. Pharmacy-related costs represented 30% of total hospitalization costs and were increased by Early-PN (+608.00 EUR/patient, p = 0.01). Notably, costs for ATC-J (anti-infective agents) (+227.00 EUR/patient, p = 0.02) and ATC-B (comprising PN) (+220.00 EUR/patient, p = 0.006) drugs were increased by Early-PN. Sensitivity analysis revealed a mean total cost increase of 1,210.00 EUR/patient (p = 0.02) by Early-PN, when incorporating the full PN costs.
The increased costs by Early-PN were mainly pharmacy-related and explained by higher expenditures for PN and anti-infective agents. The use of Early-PN in critically ill patients can thus not be recommended for both clinical (no benefit) and cost-related reasons.
ClinicalTrials.gov NCT00512122.
EPaNIC随机对照多中心试验表明,与早期肠外营养(Early-PN)相比,将重症监护病房(ICU)患者肠外营养(PN)的起始时间推迟至第一周之后(晚期PN)可促进康复。这是通过减少感染、加速器官功能衰竭的恢复以及缩短住院时间来实现的。现在,报告了从比利时医疗保健支付者角度进行的该试验预先计划的成本分析(N = 4640)。
成本数据从个体患者发票中获取。计算了索引住院期间未贴现的总医疗保健成本。构建了基于新感染的获得和住院时间延长的成本树。分析了8个成本类别对总住院成本的贡献。通过解剖治疗化学(ATC)分类系统详细阐明了药品成本的来源。在敏感性分析中探讨了Early-PN对其他医疗保健系统总住院成本的潜在影响。
发生新感染的ICU患者(24.4%)占总成本的42.7%,而住院超过一周的ICU患者(24.3%)占总成本的43.3%。与药房相关的成本占总住院成本的30%,并且因Early-PN而增加(每位患者增加608.00欧元,p = 0.01)。值得注意的是,ATC-J(抗感染药)(每位患者增加227.00欧元,p = 0.02)和ATC-B(包括PN)(每位患者增加220.00欧元,p = 0.006)药物的成本因Early-PN而增加。敏感性分析显示,纳入全部PN成本后,Early-PN使每位患者的平均总成本增加1210.00欧元(p = 0.02)。
Early-PN增加的成本主要与药房相关,原因是PN和抗感染药的支出增加。因此,出于临床(无益处)和成本相关原因,不建议在重症患者中使用Early-PN。
ClinicalTrials.gov NCT00512122。