Cardiology Division, Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts, USA.
Am J Cardiol. 2012 Sep 1;110(5):683-8. doi: 10.1016/j.amjcard.2012.04.056. Epub 2012 May 25.
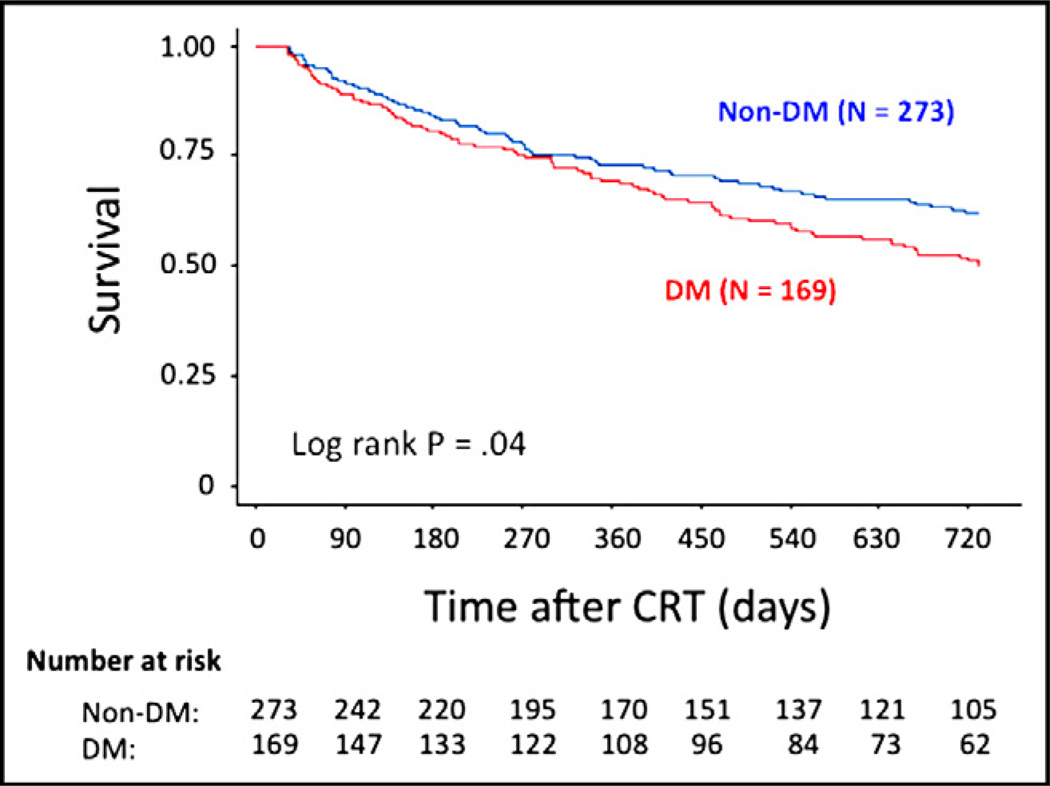
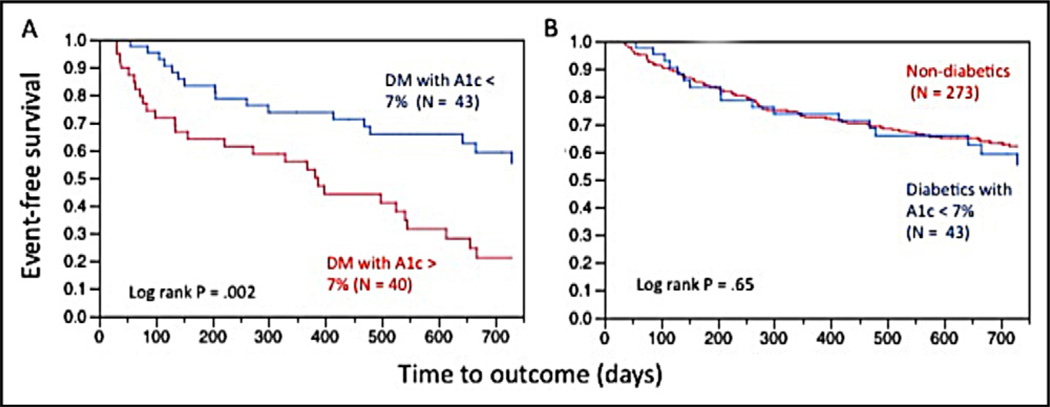
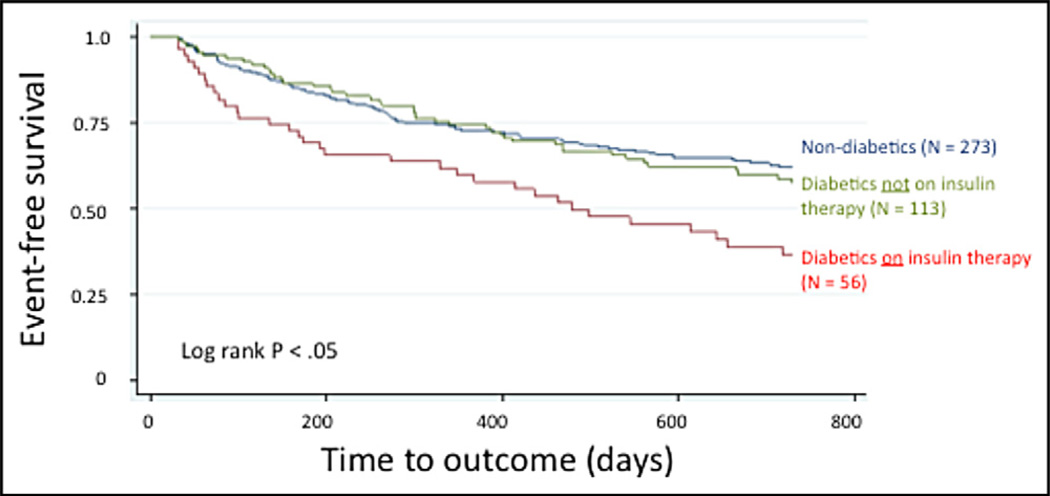
Patients with diabetes and heart failure (HF) have worse clinical outcomes compared to patients with HF without diabetes after cardiac resynchronization therapy (CRT). Patients with HF and diabetes represent a growing population at high risk for cardiovascular events and are increasingly treated with CRT. Although patients with diabetes and HF appear to benefit from CRT, their clinical outcomes are worse than those of patients without diabetes after CRT. The aim of this study was to identify clinical predictors that explain the differential hazard in patients with diabetes. We studied 442 patients (169 with diabetes) with systolic HF referred to the Massachusetts General Hospital CRT clinic from 2003 to 2010 to identify predictors of outcomes after CRT in patients with HF and diabetes. Patients with diabetes were more likely to have ischemic causes of HF than those without diabetes, but there was no difference in the left ventricular ejection fraction or HF classification at implantation. Patients with diabetes had poorer event-free survival (death or HF hospitalization) compared to those without diabetes (log-rank p = 0.04). The presence of diabetes was the most important independent predictor of differential outcomes in the entire population (hazard ratio 1.65, 95% confidence interval 1.10 to 2.51). Patients with diabetes receiving insulin therapy had poorer survival, whereas those not receiving insulin therapy had similar survival to patients without diabetes. Patients with peri-implantation glycosylated hemoglobin >7% had worse outcomes, whereas patients with glycosylated hemoglobin ≤7% had improved survival (hazard ratio 0.36, 95% confidence interval 0.15 to 0.86) equivalent to that of patients without diabetes. In conclusion, although the presence of diabetes, independent of other variables, increases the hazard of worse outcomes after CRT, there is additional risk conferred by insulin use and suboptimal peri-implantation glycemic control.
患有糖尿病和心力衰竭(HF)的患者在心脏再同步治疗(CRT)后比没有糖尿病的 HF 患者的临床结局更差。患有 HF 和糖尿病的患者代表了心血管事件风险较高的不断增长的人群,并且越来越多地接受 CRT 治疗。尽管患有糖尿病和 HF 的患者似乎从 CRT 中受益,但他们的临床结局在 CRT 后比没有糖尿病的患者更差。本研究旨在确定解释糖尿病患者差异风险的临床预测因素。我们研究了 442 名(169 名患有糖尿病)患有收缩性 HF 的患者,这些患者于 2003 年至 2010 年在马萨诸塞州综合医院 CRT 诊所就诊,以确定 HF 和糖尿病患者 CRT 后结局的预测因素。患有糖尿病的患者比没有糖尿病的患者更有可能因缺血性 HF 而就诊,但在植入时左心室射血分数或 HF 分类没有差异。与没有糖尿病的患者相比,患有糖尿病的患者无事件生存率(死亡或 HF 住院)较差(对数秩检验 p = 0.04)。在整个人群中,糖尿病的存在是差异结果的最重要独立预测因素(危险比 1.65,95%置信区间 1.10 至 2.51)。接受胰岛素治疗的糖尿病患者生存率较差,而未接受胰岛素治疗的患者与没有糖尿病的患者的生存率相似。植入后糖化血红蛋白>7%的患者结局较差,而糖化血红蛋白≤7%的患者生存状况改善(危险比 0.36,95%置信区间 0.15 至 0.86),与没有糖尿病的患者相当。总之,尽管存在糖尿病(独立于其他变量)会增加 CRT 后结局较差的风险,但胰岛素使用和植入后血糖控制不理想会带来额外的风险。