Rheumatology B Department, Paris-Descartes University, Assistance Publique Hôpitaux de Paris, Cochin Hospital, 27 rue du faubourg Saint-Jacques, Paris 14, Paris, 75014, France.
Arthritis Res Ther. 2012 May 30;14(3):R129. doi: 10.1186/ar3859.
The Rheumatoid Arthritis Impact of Disease (RAID) is a patient-reported outcome measure evaluating the impact of rheumatoid arthritis (RA) on patient quality of life. It comprises 7 domains that are evaluated as continuous variables from 0 (best) to 10 (worst). The objective was to define and identify cut-off values for disease activity states as well as improvement scores in order to present results at the individual level (for example, patient in acceptable state, improved patient).
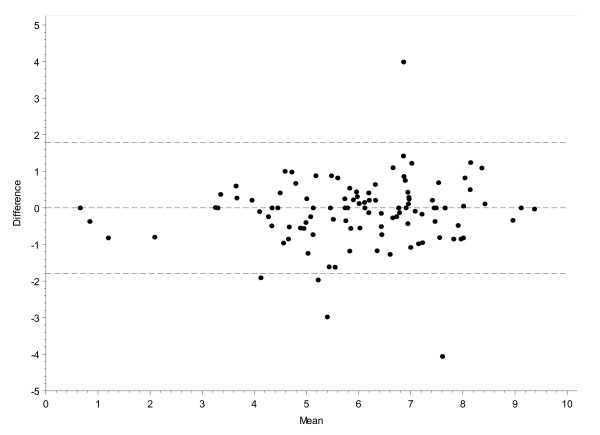
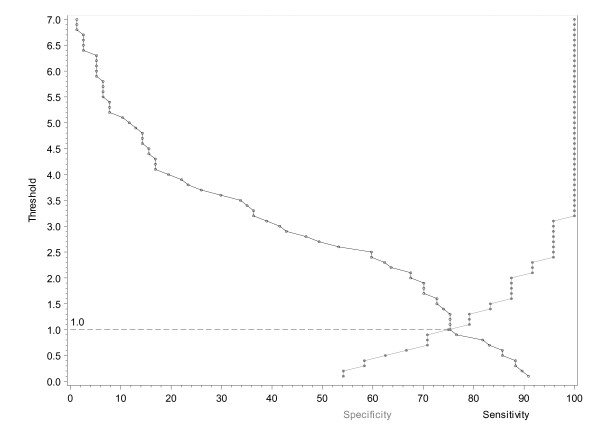
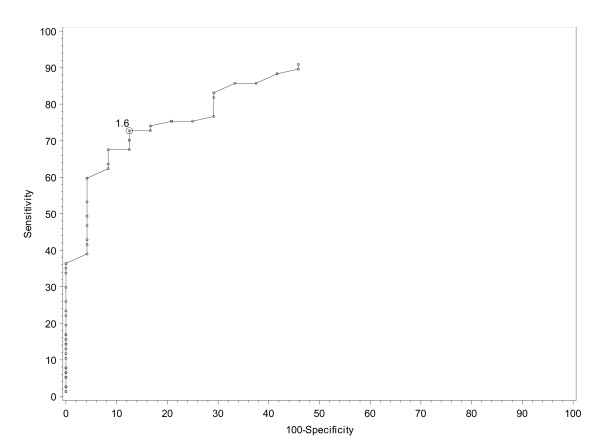
Patients with definite active RA requiring anti-tumour necrosis factor (anti-TNF) therapy were seen at screening, baseline and after 4 and 12 weeks of etanercept therapy. Answers to "Gold standard" questions on improvement (MCII: Minimum Clinically Important Improvement) and an acceptable status (PASS: Patient Acceptable Symptom State) were collected as well as the RAID score and Disease Activity Score 28- erythrocyte sedimentation rate (DAS28-ESR). Cut-offs were defined by different techniques including empirical, measurement error and gold standard anchors. The external validity of these cut-offs was evaluated using the positive likelihood ratio (LR) based on the patient's perspective (for example, patient's global) and on low disease activity status (such as DAS28-ESR).
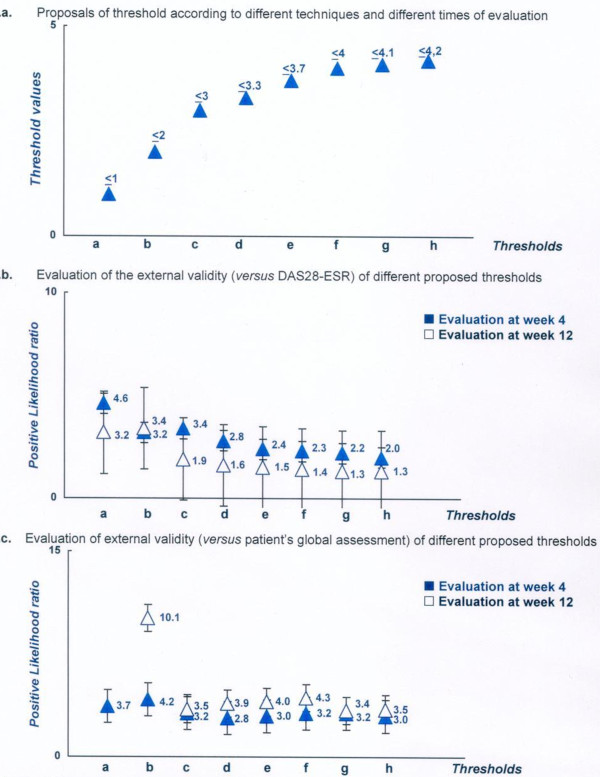
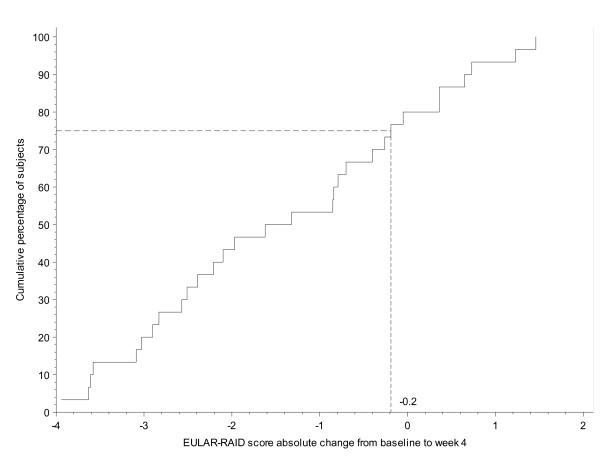
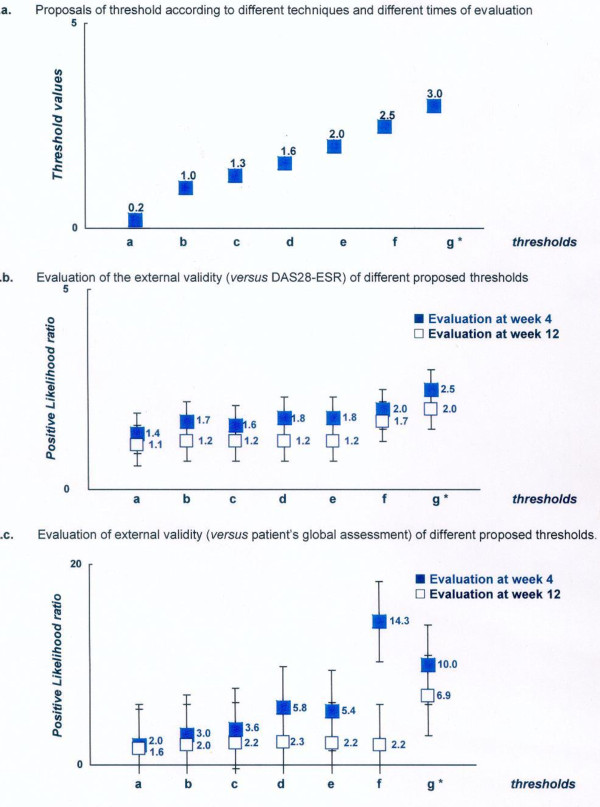
Ninety-seven (97) of the 108 recruited patients (age: 54 ± 13 years old, female gender: 75%, rheumatoid factor positive: 81%, disease duration: 8 ± 7 years, CRP: 18 ± 30 mg/l, DAS28-ESR: 5.4 ± 0.8) completed the 12 weeks of the study. The different techniques suggested thresholds ranging from 0.2 to 3 (absolute change) and from 6 to 50% (relative change) for defining MCII and thresholds from less than 1 to less than 4.2 for defining PASS. The evaluation of external validity (LR+) showed the highest LR+ was obtained with thresholds of 3 for absolute change; 50% for relative change and less than 2 for an acceptable status.
This study showed that thresholds defined for continuous variables are closely related to the methodological technique, justifying a systematic evaluation of their validity. Our results suggested that a change of at least 3 points (absolute) or 50% (relative) in the RAID score should be used to define a MCII and that a maximal value of 2 defines an acceptable status.
Clinicaltrial.gov: NCT004768053.
类风湿关节炎影响疾病(RAID)是一种评估类风湿关节炎(RA)对患者生活质量影响的患者报告结局测量工具。它由 7 个领域组成,这些领域从 0(最佳)到 10(最差)连续评估。目的是定义和确定疾病活动状态的临界值和改善分数,以便在个体水平上呈现结果(例如,可接受状态的患者,改善的患者)。
在筛查、基线以及接受依那西普治疗 4 周和 12 周后,观察到需要抗肿瘤坏死因子(抗 TNF)治疗的明确活动期 RA 患者。收集了关于改善(MCII:最小临床重要改善)和可接受状态(PASS:患者可接受症状状态)的“金标准”问题的答案,以及 RAID 评分和 28 个红细胞沉降率疾病活动度评分(DAS28-ESR)。通过不同的技术(包括经验、测量误差和金标准锚定)来定义临界值。使用基于患者观点(例如,患者的整体)和低疾病活动状态(例如 DAS28-ESR)的阳性似然比(LR)评估这些临界值的外部有效性。
在招募的 108 名患者中,有 97 名(年龄:54 ± 13 岁,女性占 75%,类风湿因子阳性占 81%,疾病持续时间:8 ± 7 年,CRP:18 ± 30mg/L,DAS28-ESR:5.4 ± 0.8)完成了 12 周的研究。不同的技术建议的 MCII 定义阈值范围为 0.2 至 3(绝对变化)和 6 至 50%(相对变化),PASS 定义的阈值范围为小于 1 至小于 4.2。外部有效性评估(LR+)显示,获得最高 LR+的阈值为绝对变化 3;相对变化 50%;可接受状态小于 2。
这项研究表明,为连续变量定义的临界值与方法学技术密切相关,需要系统地评估其有效性。我们的结果表明,RAID 评分至少变化 3 点(绝对)或 50%(相对)应用于定义 MCII,最大值 2 定义为可接受状态。
Clinicaltrial.gov:NCT004768053。