Department of Orthopaedic Surgery, Academic Medical Center, Meibergdreef 9, 1100 DD Amsterdam, The Netherlands.
Int Orthop. 2012 Sep;36(9):1923-7. doi: 10.1007/s00264-012-1585-7. Epub 2012 Jun 1.
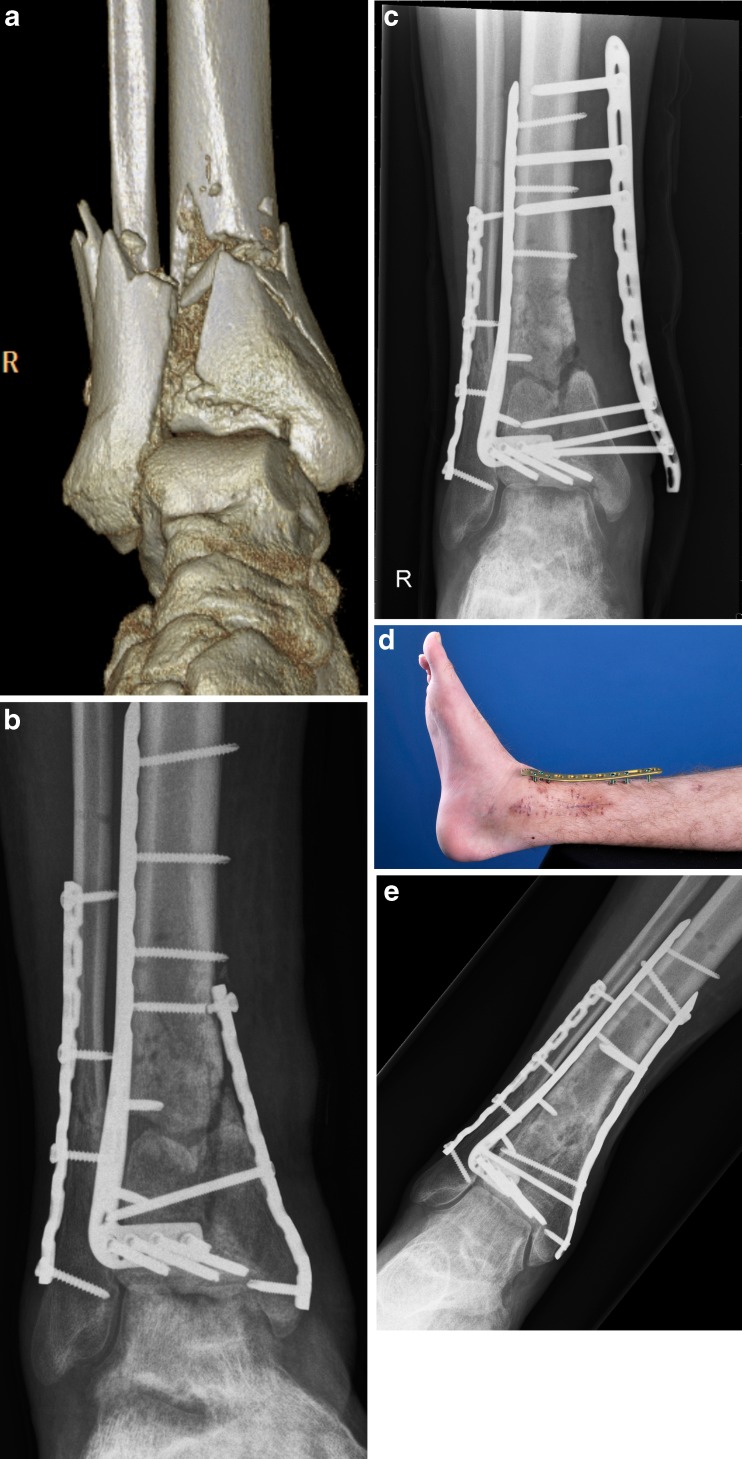
Recently we coined the term supercutaneous plating using a locking compression plate (LCP) as an external fixator. The use of this technique in peri-articular areas is facilitated by the development of anatomical plates with various screw sizes. The purpose of this report is to describe our results using the metaphyseal locking plate (LCP) as an external fixator in the treatment of infected post-traumatic problems of the distal tibia.
Between August 2008 and January 2012 a total of seven patients underwent external plating ("supercutaneous plating") of the distal tibia using a metaphyseal locking plate. Average age was 43 years (range 20-79). Six out of seven patients had a documented infection at the time of external plate application. All patients in this cohort were followed prospectively at regular intervals by the senior author (PK).
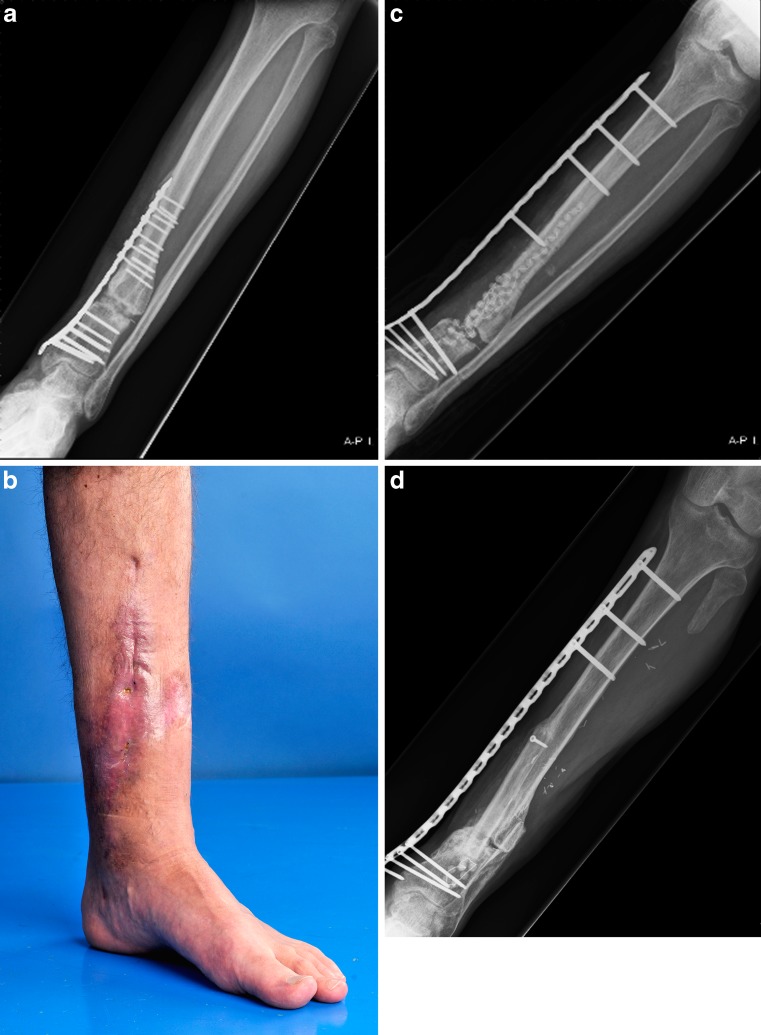
The plate was in situ for an average of 17.5 weeks (range 6-60). There were no clinically significant pin site infections. In four patients the plate was kept in place until there was complete consolidation. In three patients the external plate was exchanged for formal internal fixation once the infection had subsided. At the latest follow-up (average 12.8 months, range 4-31), all patients were fully weight bearing with a fully healed tibia. All patients were infection-free with well-healed wounds.
Infection of the distal tibia after treatment of traumatic and post-traumatic problems is a challenging problem. It is common practice that after initial debridement and hardware removal, temporary bony stabilisation is provided by external fixation. Most external frames for the lower leg are bulky and cumbersome, causing significant problems for the patient. To circumvent these issues, we have successfully used an anatomically-contoured metaphyseal locking compression plate as external fixator in a series of seven patients for acute or post-traumatic problems of the tibia.
最近,我们创造了一个术语,即使用锁定加压钢板(LCP)作为外固定器的皮下接骨术。通过开发具有各种螺钉尺寸的解剖钢板,使该技术在关节周围区域的应用更加便利。本报告的目的是描述我们使用骨干锁定钢板(LCP)作为外固定器治疗胫骨远端感染性创伤后问题的结果。
2008 年 8 月至 2012 年 1 月,共有 7 例患者接受了骨干锁定钢板的胫骨远端外固定(“皮下接骨术”)。平均年龄为 43 岁(范围 20-79 岁)。7 例中有 6 例在应用外固定器时存在明确的感染。该队列中的所有患者均由资深作者(PK)定期进行前瞻性随访。
钢板平均固定 17.5 周(范围 6-60 周)。无明显的针道感染。4 例患者在完全愈合后保留了钢板。3 例患者在感染消退后,将外固定器更换为正式的内固定。在末次随访(平均 12.8 个月,范围 4-31 个月)时,所有患者均完全负重,胫骨完全愈合。所有患者均无感染,伤口愈合良好。
创伤后和创伤后治疗的胫骨远端感染是一个具有挑战性的问题。在初次清创和去除内固定物后,临时骨稳定通常由外固定器提供,这是常见的做法。大多数小腿外固定架体积庞大,给患者带来了严重的问题。为了解决这些问题,我们在 7 例急性或创伤后胫骨问题患者中成功地使用了解剖型骨干锁定加压钢板作为外固定器。