Department of Endocrinology and Metabolism, WHO Collaborating Center for the Study and Treatment of Thyroid Diseases and Other Endocrine and Metabolic Disorders University of Pisa, Pisa, Italy.
Front Endocrinol (Lausanne). 2012 Apr 11;3:54. doi: 10.3389/fendo.2012.00054. eCollection 2012.
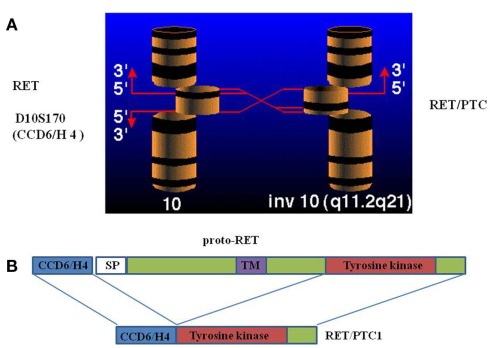
Thyroid carcinoma is the most frequent endocrine cancer accounting for 5-10% of thyroid nodules. Papillary histotype (PTC) is the most prevalent form accounting for 80% of all thyroid carcinoma. Although much is known about its epidemiology, pathogenesis, clinical, and biological behavior, the only documented risk factor for PTC is the ionizing radiation exposure. Rearrangements of the Rearranged during Transfection (RET) proto-oncogene are found in PTC and have been shown to play a pathogenic role. The first RET rearrangement, named RET/PTC, was discovered in 1987. This rearrangement constitutively activates the transcription of the RET tyrosine-kinase domain in follicular cell, thus triggering the signaling along the MAPK pathway and an uncontrolled proliferation. Up to now, 13 different types of RET/PTC rearrangements have been reported but the two most common are RET/PTC1 and RET/PTC3. Ionizing radiations are responsible for the generation of RET/PTC rearrangements, as supported by in vitro studies and by the evidence that RET/PTC, and particularly RET/PTC3, are highly prevalent in radiation induced PTC. However, many thyroid tumors without any history of radiation exposure harbor similar RET rearrangements. The overall prevalence of RET/PTC rearrangements varies from 20 to 70% of PTCs and they are more frequent in childhood than in adulthood thyroid cancer. Controversial data have been reported on the relationship between RET/PTC rearrangements and the PTC prognosis. RET/PTC3 is usually associated with a more aggressive phenotype and in particular with a greater tumor size, the solid variant, and a more advanced stage at diagnosis which are all poor prognostic factors. In contrast, RET/PTC1 rearrangement does not correlate with any clinical-pathological characteristics of PTC. Moreover, the RET protein and mRNA expression level did not show any correlation with the outcome of patients with PTC and no correlation between RET/PTC rearrangements and the expression level of the thyroid differentiation genes was observed. Recently, a diagnostic role of RET/PTC rearrangements has been proposed. It can be searched for in the mRNA extracted from cytological sample especially in case with indeterminate cytology. However, both the fact that it can be present in a not negligible percentage of benign cases and the technical challenge in extracting mRNA from cytological material makes this procedure not applicable at routine level, at least for the moment.
甲状腺癌是最常见的内分泌癌,占甲状腺结节的 5-10%。乳头状组织型(PTC)是最常见的形式,占所有甲状腺癌的 80%。尽管人们对其流行病学、发病机制、临床和生物学行为有了很多了解,但 PTC 的唯一有记录的危险因素是电离辐射暴露。在 PTC 中发现了 Rearranged during Transfection(RET)原癌基因的重排,并已证明其具有致病作用。第一个 RET 重排,命名为 RET/PTC,于 1987 年发现。这种重排使滤泡细胞中 RET 酪氨酸激酶结构域的转录持续激活,从而触发 MAPK 途径的信号传导和不受控制的增殖。到目前为止,已经报道了 13 种不同类型的 RET/PTC 重排,但最常见的两种是 RET/PTC1 和 RET/PTC3。体外研究和 RET/PTC,特别是 RET/PTC3,在辐射诱导的 PTC 中高度流行的证据表明,电离辐射是产生 RET/PTC 重排的原因。然而,许多没有任何辐射暴露史的甲状腺肿瘤也携带类似的 RET 重排。RET/PTC 重排的总发生率在 PTC 中的比例为 20%至 70%,在儿童期甲状腺癌中比成年期更为常见。关于 RET/PTC 重排与 PTC 预后之间的关系,已经有了一些有争议的数据。RET/PTC3 通常与侵袭性表型相关,特别是与更大的肿瘤大小、实性变体和更晚期的诊断阶段相关,这些都是不良预后因素。相比之下,RET/PTC1 重排与 PTC 的任何临床病理特征均无相关性。此外,RET 蛋白和 mRNA 表达水平与 PTC 患者的预后无相关性,也未观察到 RET/PTC 重排与甲状腺分化基因的表达水平之间存在相关性。最近,提出了 RET/PTC 重排的诊断作用。它可以在从细胞学样本中提取的 mRNA 中寻找,特别是在不确定的细胞学病例中。然而,它在不可忽视的良性病例中存在的事实,以及从细胞学材料中提取 mRNA 的技术挑战,使得该程序目前还不能在常规水平上应用。