Center for Clinical Epidemiology and Biostatistics, University of Pennsylvania Perelman School of Medicine, Philadelphia, PA 19104, USA.
Am J Kidney Dis. 2012 Aug;60(2):250-61. doi: 10.1053/j.ajkd.2012.04.012. Epub 2012 Jun 2.
Glomerular filtration rate (GFR) is considered the best measure of kidney function, but repeated assessment is not feasible in most research studies.
Cross-sectional study of 1,433 participants in the Chronic Renal Insufficiency Cohort (CRIC) Study (ie, the GFR subcohort) to derive an internal GFR estimating equation using a split-sample approach.
SETTING & PARTICIPANTS: Adults from 7 US metropolitan areas with mild to moderate chronic kidney disease; 48% had diabetes and 37% were black.
CRIC GFR estimating equation.
Urinary (125)I-iothalamate clearance testing (measured GFR [mGFR]).
Laboratory measures, including serum creatinine and cystatin C, and anthropometrics.
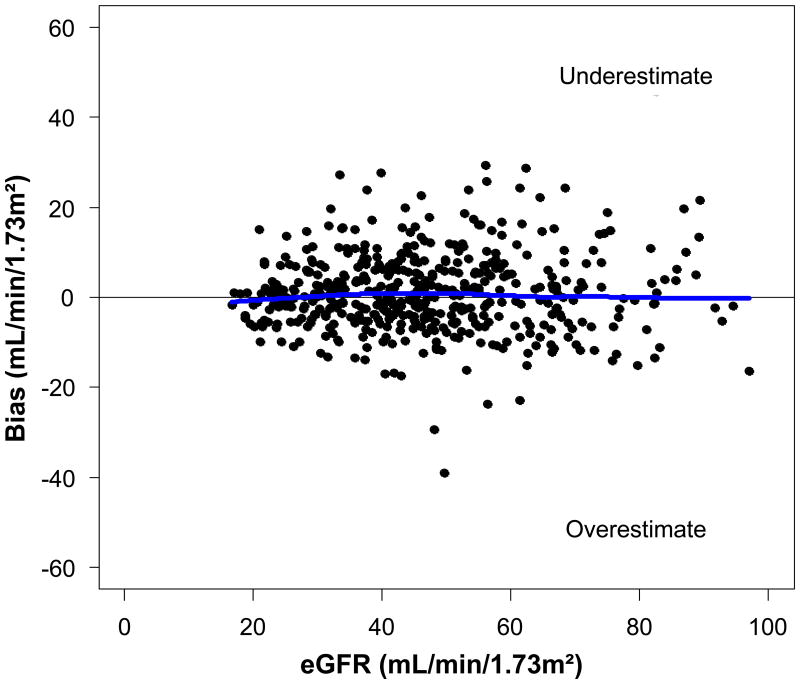
In the validation data set, the model that included serum creatinine level, serum cystatin C level, age, sex, and race was the most parsimonious and similarly predictive of mGFR compared with a model additionally including bioelectrical impedance analysis phase angle, CRIC clinical center, and 24-hour urinary creatinine excretion. Specifically, root mean square errors for the separate models were 0.207 versus 0.202, respectively. Performance of the CRIC GFR estimating equation was most accurate for the subgroups of younger participants, men, nonblacks, non-Hispanics, those without diabetes, those with body mass index <30 kg/m(2), those with higher 24-hour urine creatinine excretion, those with lower high-sensitivity C-reactive protein levels, and those with higher mGFRs.
Urinary clearance of (125)I-iothalamate is an imperfect measure of true GFR; cystatin C level is not standardized to certified reference material; lack of external validation; small sample sizes limit analyses of subgroup-specific predictors.
The CRIC GFR estimating equation predicts mGFR accurately in the CRIC cohort using serum creatinine and cystatin C levels, age, sex, and race. Its performance was best in younger and healthier participants.
肾小球滤过率(GFR)被认为是评估肾脏功能的最佳指标,但在大多数研究中,重复评估是不可行的。
对来自美国 7 个大都市地区的 1433 名慢性肾脏不全队列研究(即 GFR 亚组)参与者进行横断面研究,采用分割样本方法得出内部 GFR 估算方程。
患有轻度至中度慢性肾脏病的成年人;48%患有糖尿病,37%为黑人。
CRIC GFR 估算方程。
尿(125)I-iothalamate 清除试验(实测 GFR [mGFR])。
实验室测量,包括血清肌酐和胱抑素 C 以及人体测量学。
在验证数据集中,包含血清肌酐水平、血清胱抑素 C 水平、年龄、性别和种族的模型与另外包含生物电阻抗分析相角、CRIC 临床中心和 24 小时尿肌酐排泄的模型相比,对 mGFR 的预测更为准确。具体来说,两个模型的均方根误差分别为 0.207 和 0.202。CRIC GFR 估算方程在年龄较小的参与者、男性、非黑人、非西班牙裔、无糖尿病、体重指数(BMI)<30kg/m2、24 小时尿肌酐排泄量较高、高敏 C 反应蛋白水平较低以及 mGFR 较高的亚组中表现最为准确。
(125)I-iothalamate 的尿清除率是衡量真实 GFR 的不完美指标;胱抑素 C 水平未标准化至认证参考物质;缺乏外部验证;样本量小限制了亚组特异性预测因子的分析。
CRIC GFR 估算方程使用血清肌酐和胱抑素 C 水平、年龄、性别和种族在 CRIC 队列中准确预测 mGFR。其性能在较年轻和健康的参与者中最佳。