Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland.
Children's Hospital of Philadelphia, Philadelphia, Pennsylvania; Department of Pediatrics, Division of Nephrology, Perelman School of Medicine, University of Pennsylvania, Philadelphia, Pennsylvania.
Am J Kidney Dis. 2022 Aug;80(2):174-185.e1. doi: 10.1053/j.ajkd.2021.10.013. Epub 2021 Dec 30.
RATIONALE & OBJECTIVE: Recent reassessment of the use of race in estimated glomerular filtration rate (eGFR) in adults has instigated questions about the role of race in eGFR expressions for children. Little research has examined the associations of self-reported race with measured GFR (mGFR) adjusting for serum creatinine or cystatin C in children and young adults with chronic kidney disease (CKD). This study examined these associations and evaluated the performance of the previously published "U25" (under the age of 25 years) eGFR equations in a large cohort of children and young adults with CKD.
Observational cohort study.
SETTING & PARTICIPANTS: Participants in the Chronic Kidney Disease in Children (CKiD) study including 190 Black and 675 non-Black participants contributing 473 and 1,897 annual person-visits, respectively.
Self- or parental-reported race (Black, non-Black). Adjustment for serum creatinine or cystatin C, body size, and socioeconomic status.
mGFR based on iohexol clearance.
Linear regression with generalized estimating equations, stratified by age (<6, 6-12, 12-18, and ≥18 years) incorporating serum creatinine or serum cystatin C. Contrasting performance in different self-reported racial groups of the U25 eGFR equations.
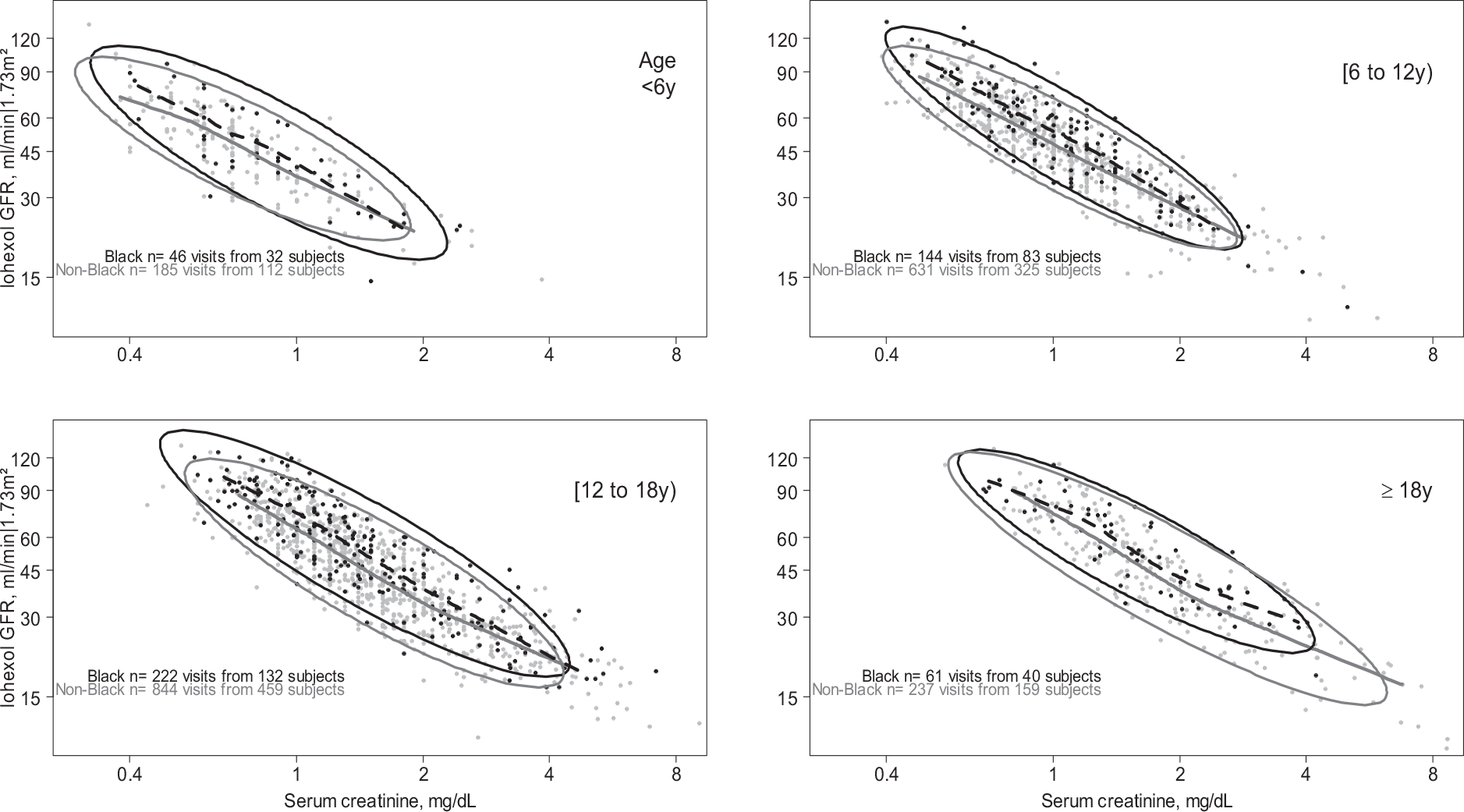
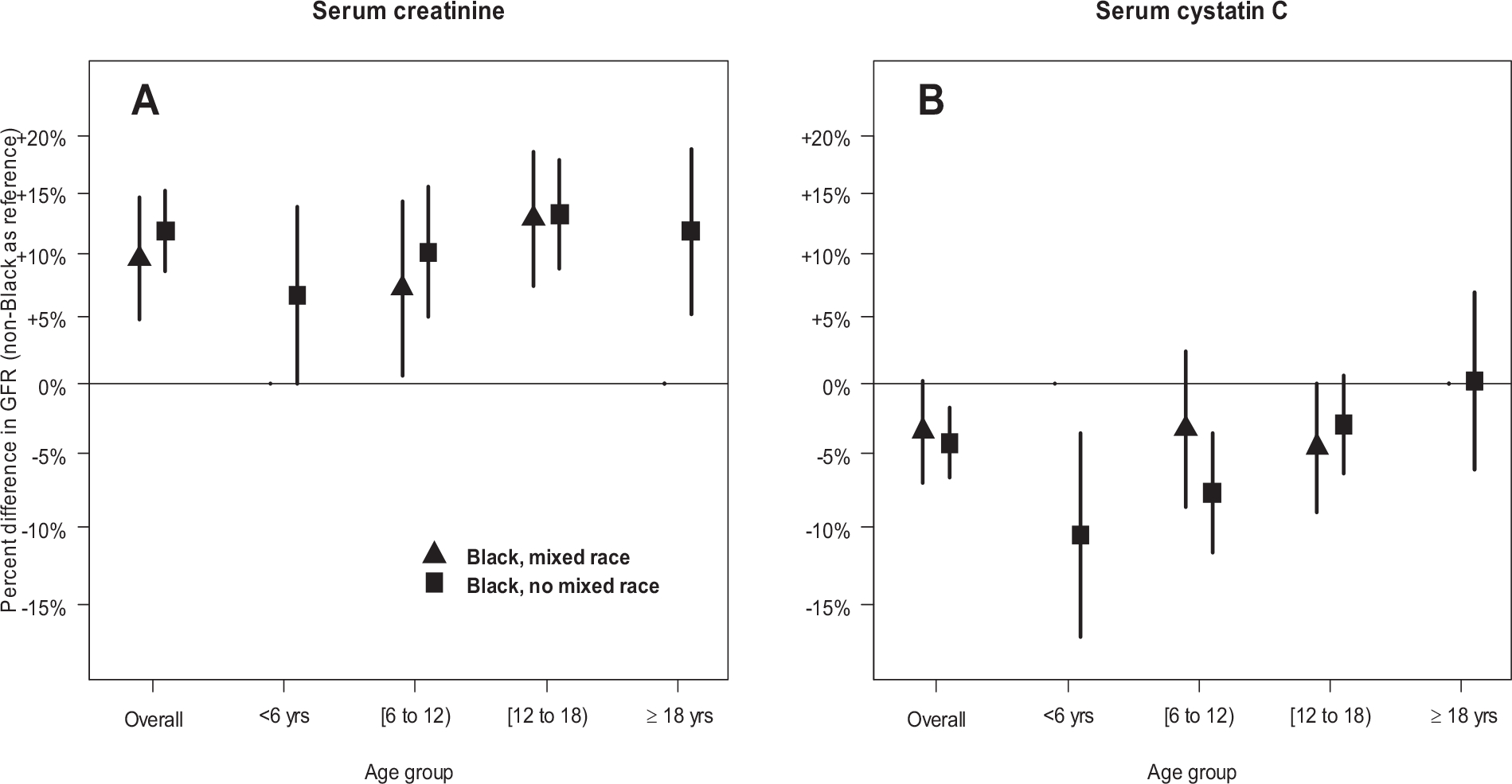
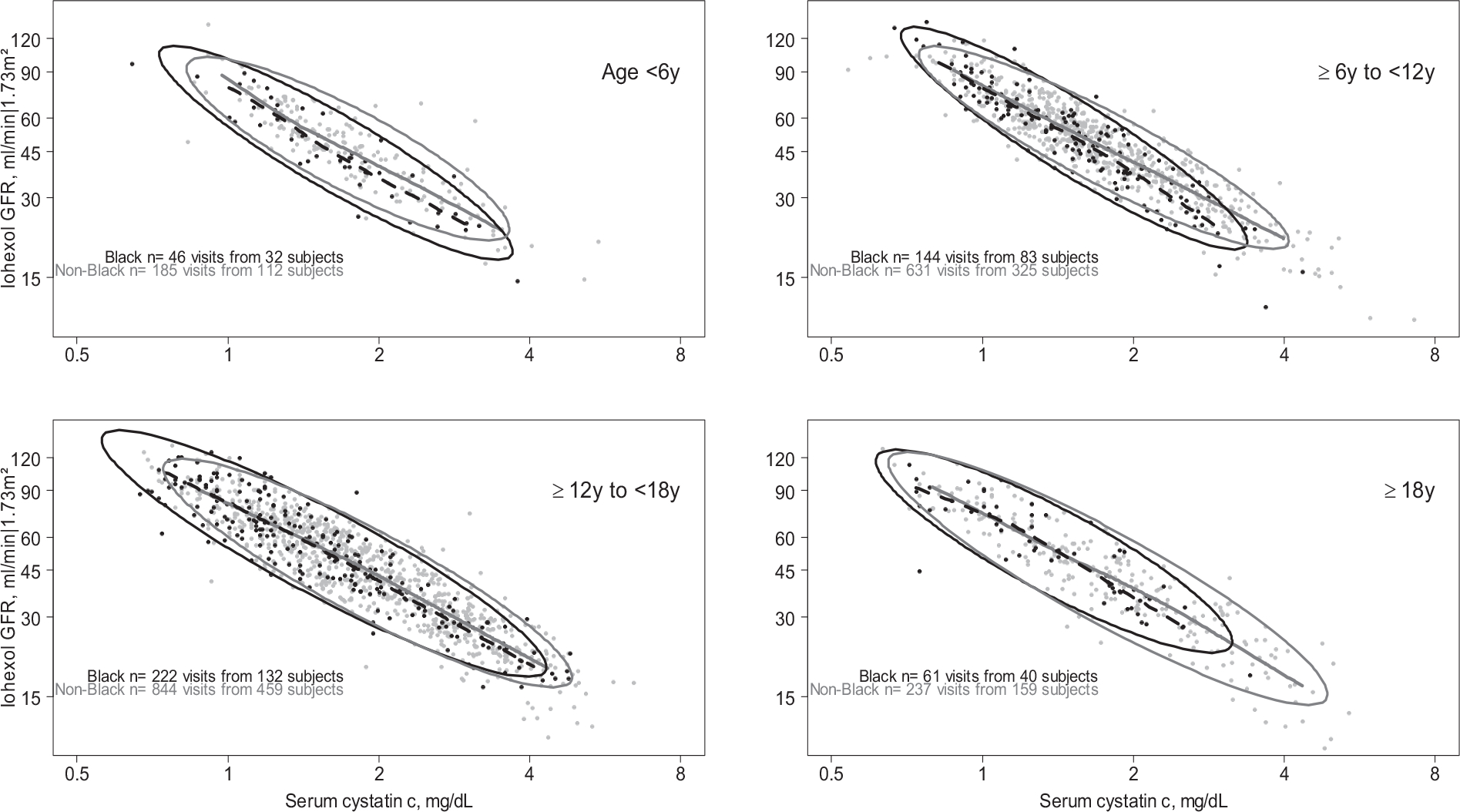
Self-reported Black race was significantly associated with 12.8% higher mGFR among children in regression models including serum creatinine. Self-reported Black race was significantly associated with 3.5% lower mGFR after adjustment for cystatin C overall but was not significant for those over 12 years. The results were similar after adjustment for body size and socioeconomic factors. The average of creatinine- and cystatin C-based U25 equations was unbiased by self-reported race groups.
Small number of children < 6 years; lean body mass was estimated.
Differences in the creatinine-mGFR relationship by self-reported race were observed in children and young adults with CKD and were consistent with findings in adults. Smaller and opposite differences were observed for the cystatin C-mGFR relationship, especially in the younger age group. We recommend inclusion of children for future investigations of biomarkers to estimate GFR. Importantly, for GFR estimation among those under 25 years of age, the average of the new U25 creatinine and cystatin C equations without race coefficients yields unbiased estimates of mGFR.
最近对成年人肾小球滤过率(eGFR)中种族使用的重新评估引发了关于种族在儿童 eGFR 表达中作用的问题。很少有研究调查自我报告的种族与通过测量肾小球滤过率(mGFR)与血清肌酐或胱抑素 C 相关联,在患有慢性肾脏病(CKD)的儿童和年轻人中。本研究检验了这些关联,并评估了之前发表的“U25”(25 岁以下)eGFR 方程在患有 CKD 的大量儿童和年轻人中的表现。
观察性队列研究。
慢性肾脏病儿童(CKiD)研究的参与者,包括 190 名黑人参与者和 675 名非黑人参与者,分别提供了 473 年和 1897 年的年度人次就诊。
自我报告或父母报告的种族(黑人,非黑人)。调整血清肌酐或胱抑素 C、体型和社会经济地位。
基于 iohexol 清除率的 mGFR。
使用广义估计方程的线性回归,按年龄(<6、6-12、12-18 和≥18 岁)分层,包含血清肌酐或血清胱抑素 C。对比 U25 eGFR 方程在不同自我报告的种族群体中的表现。
在包含血清肌酐的回归模型中,自我报告的黑人种族与儿童 mGFR 高 12.8%显著相关。在调整胱抑素 C 后,整体上自我报告的黑人种族与 mGFR 低 3.5%相关,但在 12 岁以上人群中不显著。在调整体型和社会经济因素后,结果相似。基于肌酐和胱抑素 C 的 U25 方程的平均值不受自我报告的种族群体的影响。
<6 岁的儿童人数较少;瘦体重是估计的。
在患有 CKD 的儿童和年轻人中,自我报告的种族与肌酐-mGFR 关系存在差异,与成年人的发现一致。胱抑素 C-mGFR 关系的差异较小且相反,尤其是在年龄较小的组中。我们建议纳入儿童参与未来对生物标志物的 GFR 估计的研究。重要的是,对于 25 岁以下人群的 GFR 估计,不包含种族系数的新 U25 肌酐和胱抑素 C 方程的平均值可以产生 mGFR 的无偏估计。