Heart and Vascular Institute, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195, USA.
Eur Heart J. 2012 Sep;33(17):2189-96. doi: 10.1093/eurheartj/ehs121. Epub 2012 Jun 7.
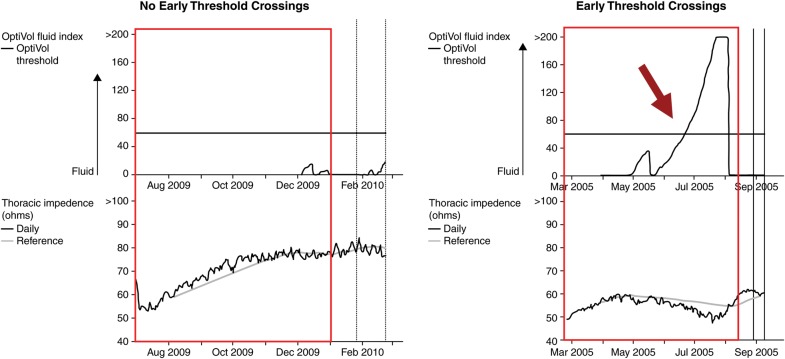
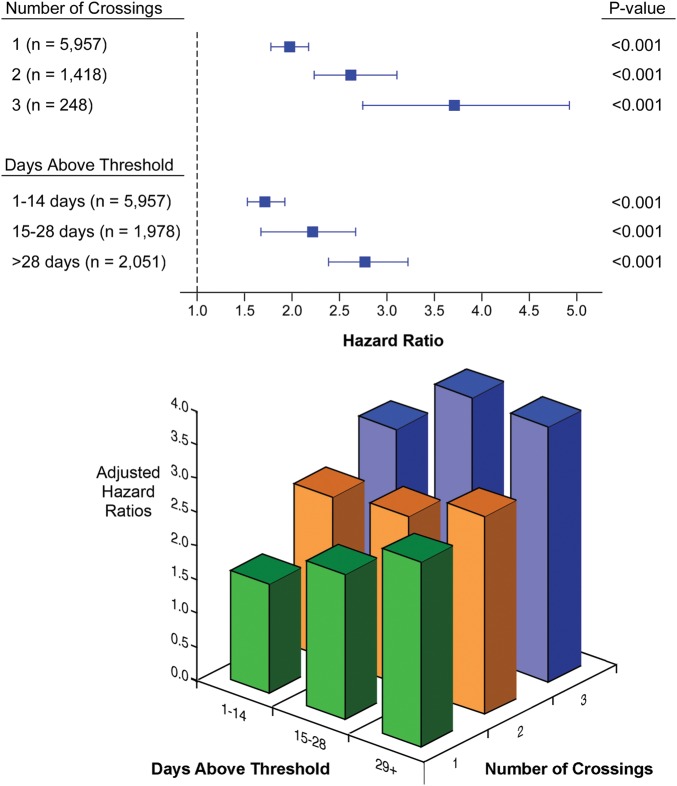
Threshold crossings of impedance trends detected by implanted devices have been associated with clinically relevant heart failure events, but long-term prognosis of such events has not been demonstrated. The aim of this study is to examine the relationship between alterations in intrathoracic impedance and mortality risk in patients with implantable devices.
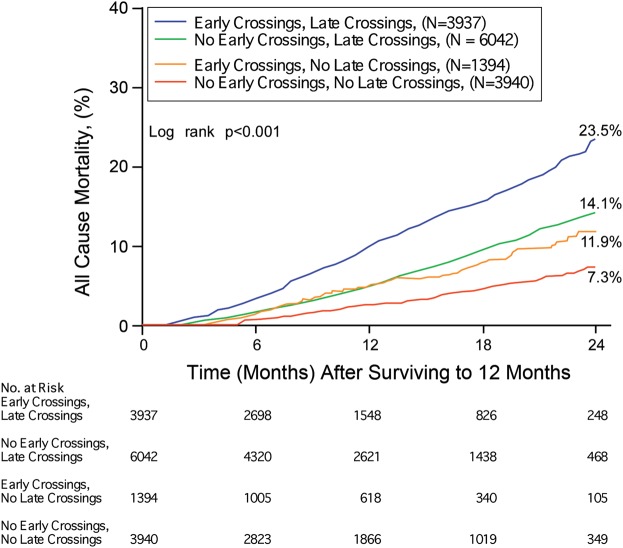
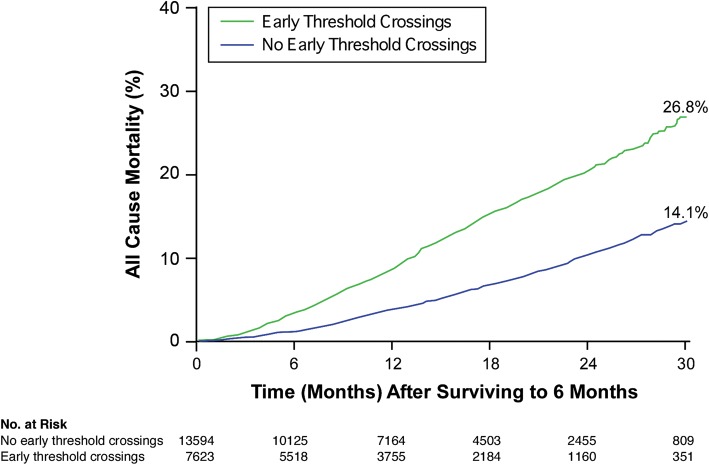
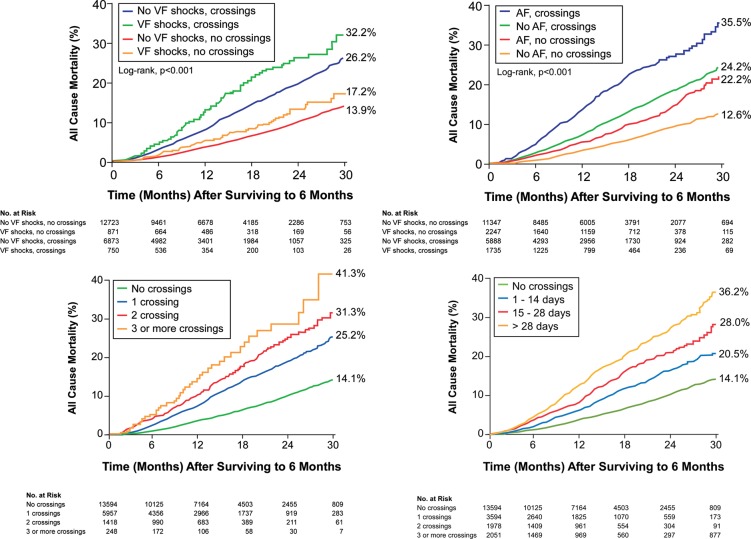
We reviewed remote monitoring data in the de-identified Medtronic CareLink(®) Discovery Link that captured intrathoracic impedance trends for >6 months. The initial 6 months of the cardiac and impedance trends were used as the observation period to create the patient groups and cross-referenced with the Social Security Death Index for mortality data. In our study cohort of 21 217 patients, 36% experienced impedance threshold crossing within the initial 6 months of monitoring (defined as the 'early threshold crossing' group). Patients with early threshold crossings demonstrated an increased risk of age- and gender-adjusted all-cause mortality [hazard ratio (HR) 2.15, 95% confidence interval (CI) 1.95-2.38, P< 0.0001]. Increased mortality risk remained significant when analysed in subgroups of patients without defibrillator shock (HR 2.10, 95% CI 1.90-2.34, P< 0.0001, n= 1621) or within those patients without device-detectable atrial fibrillation (AF) during the initial 6 months of monitoring (HR 2.09, 95% CI 1.86-2.34, P< 0.0001, n= 17 235). Both the number and the duration of early threshold crossings of impedance trends detectable by implanted devices were associated with increased mortality risk. Furthermore, the improvement of altered impedance trends portends more favourable prognosis.
Threshold crossing of impedance trends detectable by implanted devices is associated with relatively increased mortality risk even after adjusted for demographic, device-detected AF, or defibrillator shocks.
植入设备检测到的阻抗趋势的阈值交叉已与临床相关的心力衰竭事件相关,但尚未证明此类事件的长期预后。本研究旨在检查植入设备患者的胸腔内阻抗变化与死亡率风险之间的关系。
我们回顾了 Medtronic CareLink(®)Discovery Link 中去识别的远程监测数据,该数据捕获了胸腔内阻抗趋势超过 6 个月。心脏和阻抗趋势的最初 6 个月被用作观察期,以创建患者组,并与社会保障死亡指数交叉引用以获取死亡率数据。在我们的 21217 名患者的研究队列中,36%的患者在监测的最初 6 个月内经历了阻抗阈值交叉(定义为“早期阈值交叉”组)。早期阈值交叉的患者具有较高的年龄和性别调整后全因死亡率风险[风险比(HR)2.15,95%置信区间(CI)1.95-2.38,P<0.0001]。当在没有除颤器电击的患者亚组中进行分析(HR 2.10,95%CI 1.90-2.34,P<0.0001,n=1621)或在监测的最初 6 个月内没有设备检测到心房颤动(AF)的患者中进行分析时,死亡率风险仍然显著(HR 2.09,95%CI 1.86-2.34,P<0.0001,n=17235)。植入设备检测到的阻抗趋势的早期阈值交叉的数量和持续时间均与死亡率风险增加相关。此外,改变的阻抗趋势的改善预示着更好的预后。
即使在调整了人口统计学,设备检测到的 AF 或除颤器电击后,植入设备检测到的阻抗趋势的阈值交叉仍与相对增加的死亡率风险相关。