Departement of Surgery, ASL10, Ospedale San Giovanni di Dio, Florence, Italy.
J Orthop Traumatol. 2012 Sep;13(3):125-30. doi: 10.1007/s10195-012-0199-6. Epub 2012 Jun 13.
Fixation of pertrochanteric fracture is undoubtedly an additional trauma after the fracture itself. In elderly patients, it might have an important impact on the whole organism. In the literature we find various techniques to perform this type of surgery. Up to now, there are no parameters validated for quantification of the invasiveness of a surgical procedure; it is therefore still not demonstrated that any method is less invasive than any other. In an effort to find a way to quantify the invasiveness of a surgical procedure, inflammatory markers were collected in patients undergoing fixation of trochanteric fracture with gliding hip screw [dynamic hip screw (DHS)] using either a conventional (DHS conv) or minimally invasive (DHS MIO) technique.
Two groups of patients were investigated prospectively; 36 of them were treated with conventional DHS technique and 32 with minimally invasive technique. Mean age was 84.7 ± 7.20 and 82.78 ± 7.71 years, respectively. Fracture type was classified according to the AO classification. Interleukin (IL)-6, IL-10, IL-8, and tumor necrosis factor (TNF)-α were measured 1 h before and 1 h after surgery. Student's t test, chi-square test, and multivariate logistic regression were used for statistical analysis.
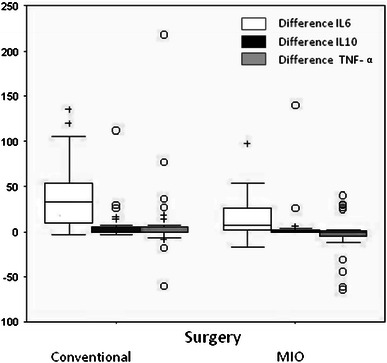
Preoperative levels of interleukins showed no significant differences between the two groups. In contrast, the postoperative blood level of IL-6 in patients operated with DHS conv technique (78.41 ± 67.04 pg/ml) was on average higher than in patients operated by DHS MIO technique (39.02 ± 37.36 pg/ml), the mean difference being 39.39 pg/ml [95 % confidence interval (CI) 12.65-66.13 pg/ml; p = 0.0045]. Multivariate logistic regression (backward method with limit of significance 0.05) confirmed that patients operated by conventional technique were significantly more likely to have increased IL-6 after surgery than those operated by MIO technique. IL-8 was measured in only 36 patients (20 for DHS conv, 16 for DHS MIO). No significant differences were found between the two groups; however, there was a drastic decrease postoperatively (p < 0.0001) regardless of the type of surgery performed. IL-10 and TNF-α were tested in all subjects, but did not show significant differences between the two groups. Average length of incision was significantly different (4.61 cm, 95 % CI 3.50-5.71 cm; p < 0.001) between the two groups, being 11.65 ± 2.64 cm for DHS conv and 7.05 ± 1.77 cm for DHS MIO. Similarly, average units of red blood cells (RBCs) transfused [performed for hemoglobin (Hb) <9 g/dl and/or hematocrit (HCT) <27 %] was higher (2.22 ± 0.99) in the DHS conv group compared with the DHS MIO group (1.09 ± 1.20), with average difference of 1.13 (95 % CI 0.59-1.66; p < 0.001).
This attempt to quantify the invasiveness of internal fixation for trochanteric fracture comparing two techniques (DHS conv versus DHS MIO) based on inflammatory markers (IL-6) has given encouraging results. Measurement of systemic inflammatory response to local tissue damage caused by osteosynthesis using IL-6 as marker seems to confirm the lower invasiveness of MIO techniques. These results for trauma cases seem in line with those published for hip prosthesis. Ongoing further studies analyzing the effect of nailing will confirm or invalidate these preliminary results.
股骨转子间骨折固定本身无疑是骨折后的又一次创伤。在老年患者中,它可能对整个机体产生重要影响。在文献中,我们发现了各种进行此类手术的技术。到目前为止,还没有用于量化手术侵袭性的参数;因此,仍然不能证明任何方法比其他方法更具侵袭性。为了找到量化手术侵袭性的方法,我们收集了使用滑动髋螺钉(动力髋螺钉 [DHS])固定转子间骨折的患者的炎症标志物,这些患者分别接受了常规(DHS 常规)或微创(DHS MIO)技术治疗。
前瞻性地研究了两组患者;其中 36 例接受常规 DHS 技术治疗,32 例接受微创技术治疗。平均年龄分别为 84.7 ± 7.20 岁和 82.78 ± 7.71 岁。骨折类型根据 AO 分类进行分类。在手术前 1 小时和手术后 1 小时测量白细胞介素(IL)-6、IL-10、IL-8 和肿瘤坏死因子(TNF)-α。使用 Student's t 检验、卡方检验和多变量逻辑回归进行统计学分析。
两组患者术前白细胞介素水平无显著差异。相反,接受 DHS conv 技术手术的患者术后 IL-6 血水平(78.41 ± 67.04 pg/ml)平均高于接受 DHS MIO 技术手术的患者(39.02 ± 37.36 pg/ml),平均差异为 39.39 pg/ml [95%置信区间(CI)12.65-66.13 pg/ml;p = 0.0045]。多变量逻辑回归(显著性水平为 0.05 的后向法)证实,接受常规技术手术的患者术后 IL-6 升高的可能性明显高于接受 MIO 技术手术的患者。仅对 36 例患者进行了 IL-8 测量(DHS conv 20 例,DHS MIO 16 例)。两组之间没有发现显著差异;然而,无论手术类型如何,术后都急剧下降(p <0.0001)。所有患者均检测了 IL-10 和 TNF-α,但两组之间没有显著差异。切口平均长度有显著差异(4.61 cm,95%CI 3.50-5.71 cm;p <0.001),DHS conv 组为 11.65 ± 2.64 cm,DHS MIO 组为 7.05 ± 1.77 cm。同样,接受 DHS conv 治疗的患者平均输血量(血红蛋白 [Hb] <9 g/dl 和/或血细胞比容 [HCT] <27%时进行)也高于 DHS MIO 组(1.09 ± 1.20),平均差异为 1.13(95%CI 0.59-1.66;p <0.001)。
这项尝试通过炎症标志物(IL-6)比较两种技术(DHS conv 与 DHS MIO)来量化转子间骨折内固定的侵袭性的尝试取得了令人鼓舞的结果。使用 IL-6 作为标志物测量骨合成术引起的局部组织损伤的全身炎症反应似乎证实了 MIO 技术的较低侵袭性。这些创伤病例的结果似乎与发表的髋关节假体结果一致。正在进行的进一步分析锁定接骨术影响的研究将证实或否定这些初步结果。