Cochlear Bone Anchored Solutions, Gothenburg, Sweden.
Clin Exp Otorhinolaryngol. 2012 Apr;5 Suppl 1(Suppl 1):S43-7. doi: 10.3342/ceo.2012.5.S1.S43. Epub 2012 Apr 30.
Variability in Baha® sound processor fittings may arise from the nature of the implant-to-bone transmission as well as transcranial attenuation for patients with single-sided sensorineural deafness (SSD). One method of improving the predictability of Baha fittings is to measure the individual patient's actual bone conduction thresholds, thereby removing the influences of skin thickness and/or the implant location site.
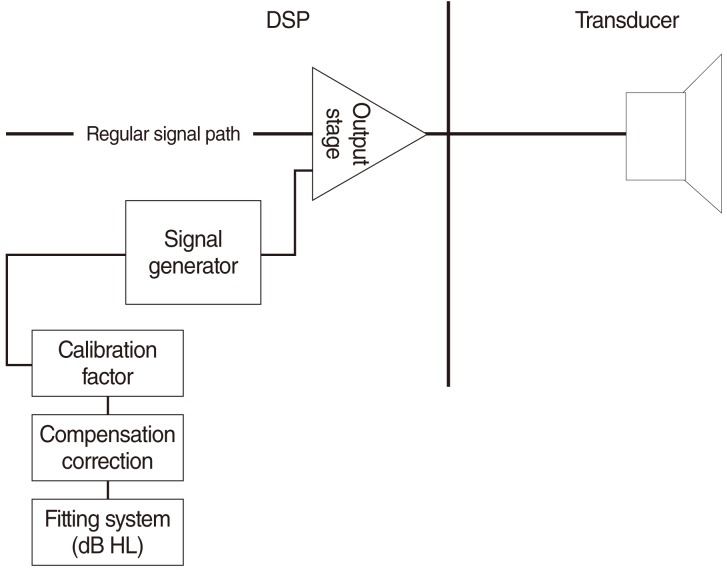
Twenty adult wearers of the Baha bone conduction implant system participated in the study. Direct bone conduction thresholds were obtained through the BC Direct function of the Baha Fitting Software combined with the Cochlear Baha BP100 sound processor. For comparison, the masked and unmasked bone conduction responses of the patients were collected through standard audiometric testing techniques. Test-retest reliability measurement was performed for all participants. Data for each frequency and frequency range were analyzed separately.
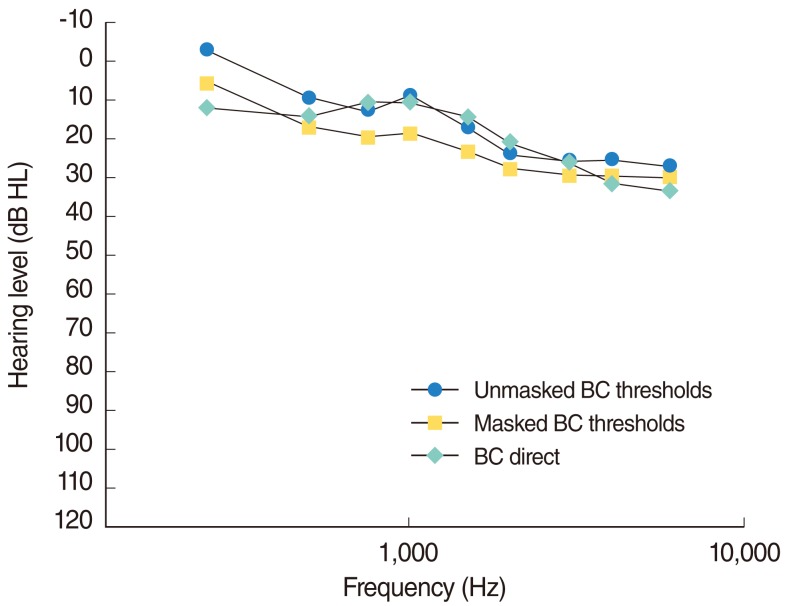
The results confirm the improved transmission of sound through the implant rather than transcutaneously through the skin. On average, the BC Direct thresholds were closer to the patient's unmasked thresholds than the masked values. In subjects with SSD, BC Direct results were poorer than contra-lateral bone conduction thresholds, most likely due to transcranial attenuation. The test-retest reliability for the BC Direct measurements was within +/-5 dB. The comparison of preferred amplification, based on direct bone conduction or bone conduction audiometry, found higher agreement for fittings based on direct bone conduction measurements.
While the transfer function between the implant and the skin can be predicted on average, there are a number of patients for whom measurement is essential to determine the required amplification. These were patients with: 1) SSD, 2) asymmetrical hearing loss, 3) unusual implant location or skull formation, and 4) users of Testband or Softband. The result for the clinician is that a fitting can take place with less fine-tuning and a greater understanding of the variability of bone conducted sound transmission.
对于单侧感音神经性聋(SSD)患者,由于骨导植入物向颅骨的传输以及颅外衰减的性质,Baha® 声音处理器的适配可能存在差异。提高 Baha 适配可预测性的一种方法是测量个体患者的实际骨导阈值,从而消除皮肤厚度和/或植入物位置的影响。
本研究纳入了 20 名成年 Baha 骨导植入系统佩戴者。直接骨导阈值通过 Cochlear Baha BP100 声音处理器与 Baha 拟合软件的 BC Direct 功能联合获得。为了进行比较,通过标准听力测试技术收集了患者的掩蔽和未掩蔽骨导反应。所有参与者均进行了测试-重测可靠性测量。分别分析了每个频率和频率范围的数据。
结果证实了声音通过植入物而不是通过皮肤经皮传输的改善。平均而言,BC Direct 阈值比掩蔽值更接近患者的未掩蔽阈值。在 SSD 患者中,BC Direct 结果比对侧骨导阈值差,这很可能是由于颅外衰减所致。BC Direct 测量的测试-重测可靠性在 +/-5dB 以内。基于直接骨导或骨导测听的首选放大比较发现,基于直接骨导测量的适配具有更高的一致性。
虽然可以平均预测植入物和皮肤之间的传递函数,但对于某些患者,测量对于确定所需放大至关重要。这些患者包括:1)SSD,2)听力损失不对称,3)植入物位置或颅骨形态异常,4)Testband 或 Softband 用户。这一结果对临床医生来说意味着,适配可以在减少微调的情况下进行,并更好地理解骨导声音传输的可变性。