Harnalikar Manoj, Kharkar Vidya, Khopkar Uday
Departments of Dermatology, Venereology, and Leprology, Seth G.S. Medical College and KEM Hospital, Mumbai, India.
Indian J Dermatol. 2012 May;57(3):206-9. doi: 10.4103/0019-5154.96194.
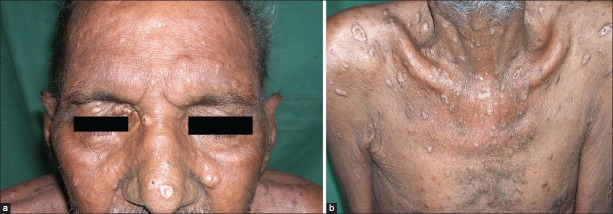
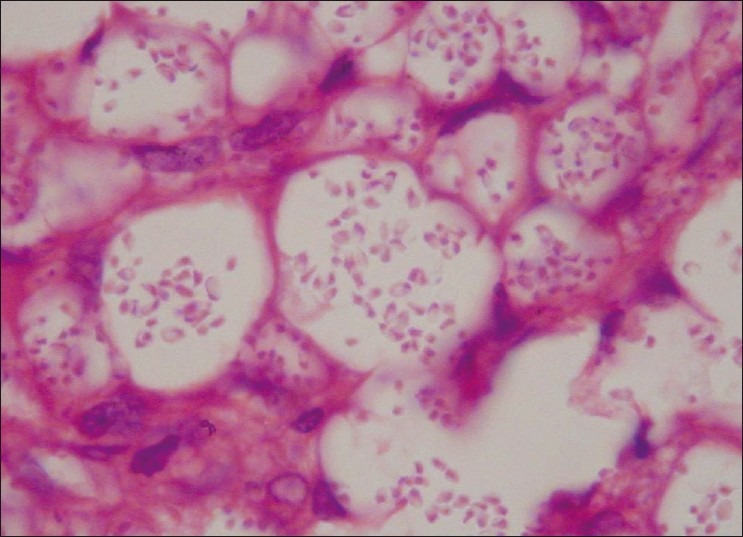
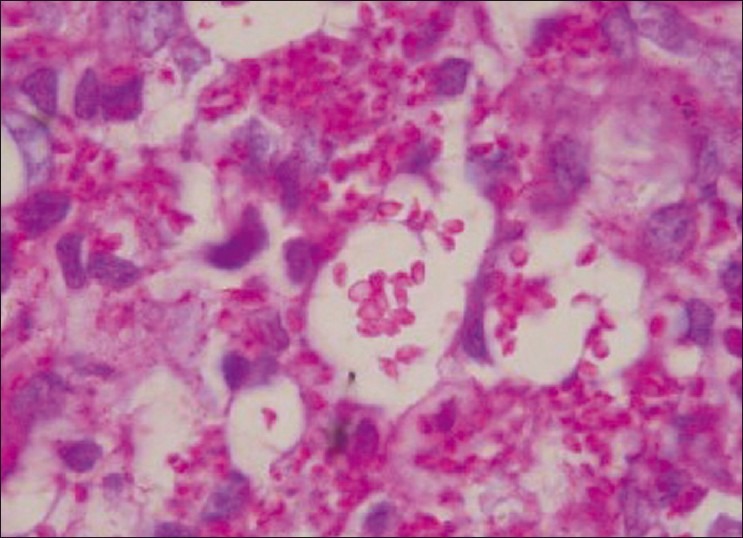
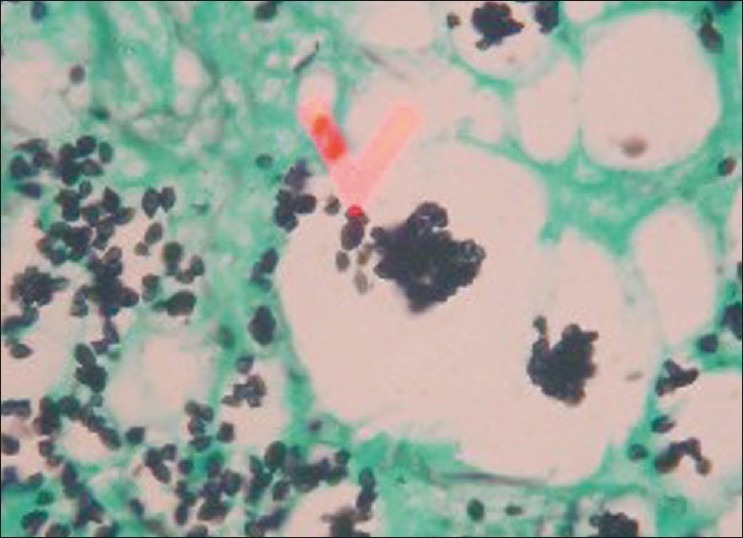
Histoplasmosis, a systemic mycosis caused by the dimorphic fungus Histoplasma capsulatum var capsulatum and Histoplasma capsulatum var duboisii is endemic to many parts of the world. The clinical manifestations range from acute or chronic pulmonary infection to a progressive disseminated disease. After initial exposure to the fungus, the infection is self-limited and restricted to the lungs in 99% of healthy individuals. The remaining 1%, however, progress to either disseminated or chronic disease involving the lungs, liver, spleen, lymph nodes, bone marrow or rarely, the skin and mucous membranes. Mucocutaneous histoplasmosis is frequently reported in patients with acquired immune deficiency syndrome (AIDS), but it is rare in immunocompetent hosts. A 60-year-old male presented with asymptomatic swelling of the hard palate and crusted papules and nodules over the extremities, face and trunk. Clinically, the diagnoses of cutaneous cryptococcosis versus histoplasmosis was considered in this patient. A chest X-ray revealed hilar lymphadenopathy. Enzyme-linked immunosorbent assay (ELISA) for human immunodeficiency virus (HIV) was nonreactive. Skin biopsy revealed multiple tiny intracellular round yeast forms with a halo in the mid-dermis. Culture of the skin biopsy in Sabouraud's dextrose agar showed colonies of Histoplasma capsulatum. Despite an investigation including no evidence of underlying immunosuppression was found, he was started on IV amphotericin-B (0.5 mg/kg/day). However, the patient succumbed to his disease 2 days after presentation. We report a rare case of disseminated cutaneous histoplasmosis in an immunocompetent individual.
组织胞浆菌病是一种由双相真菌荚膜组织胞浆菌荚膜变种和荚膜组织胞浆菌杜波依斯变种引起的全身性真菌病,在世界许多地区均有流行。其临床表现从急性或慢性肺部感染到进行性播散性疾病不等。初次接触该真菌后,99%的健康个体感染为自限性且局限于肺部。然而,其余1%会发展为累及肺部、肝脏、脾脏、淋巴结、骨髓的播散性或慢性疾病,皮肤和黏膜受累则较为罕见。皮肤黏膜组织胞浆菌病在获得性免疫缺陷综合征(AIDS)患者中经常报道,但在免疫功能正常的宿主中罕见。一名60岁男性出现硬腭无症状肿胀以及四肢、面部和躯干有结痂丘疹和结节。临床上,该患者被考虑诊断为皮肤隐球菌病与组织胞浆菌病。胸部X线显示肺门淋巴结肿大。人类免疫缺陷病毒(HIV)酶联免疫吸附测定(ELISA)为阴性。皮肤活检显示真皮中部有多个微小的细胞内圆形酵母样形态,周围有晕环。皮肤活检组织在沙氏葡萄糖琼脂培养基上培养显示有荚膜组织胞浆菌菌落。尽管进行了调查,未发现潜在免疫抑制的证据,但仍开始给予静脉注射两性霉素B(0.5mg/kg/天)。然而,患者在就诊后2天死于该病。我们报告了一例免疫功能正常个体发生播散性皮肤组织胞浆菌病的罕见病例。