Kang Shin Kwang, Lee Seokkee, Oh Hyun Kong, Kang Min-Woong, Na Myung Hoon, Yu Jae Hyeon, Koo Bon Seok, Lim Seung Pyung
Department of Thoracic and Cardiovascular Surgery, Chungnam National University Hospital, Chungnam National University School of Medicine, Korea.
Korean J Thorac Cardiovasc Surg. 2012 Jun;45(3):171-6. doi: 10.5090/kjtcs.2012.45.3.171. Epub 2012 Jun 7.
Deep neck infections (DNI) can originate from infection in the potential spaces and fascial planes of the neck. DNI can be managed without surgery, but there are cases that need surgical treatment, especially in the case of mediastinal involvement. The aim of this study is to identify clinical features of DNI and analyze the predisposing factors for mediastinal extension.
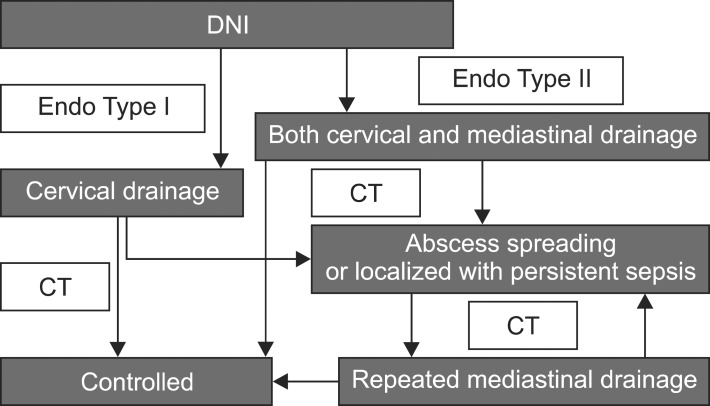
We reviewed medical records of 56 patients suffering from DNI who underwent cervical drainage only (CD group) and those who underwent cervical drainage combined with mediastinal drainage for descending necrotizing mediastinitis (MD group) from August 2003 to May 2009 and compared the clinical features of each group and the predisposing factors for mediastinal extension.
Forty-four out of the 56 patients underwent cervical drainage only (79%) and 12 patients needed both cervical and mediastinal drainage (21%). There were no differences between the two groups in gender (p=0.28), but the MD group was older than the CD group (CD group, 44.2±23.2 years; MD group, 55.6±12.1 years; p=0.03). The MD group had a higher rate of co-morbidity than the CD group (p=0.04). The CD group involved more than two spaces in 14 cases (32%) and retropharyngeal involvement in 12 cases (27%). The MD group involved more than two spaces in 11 cases (92%) and retropharyngeal involvement in 12 cases (100%). Organism identification took place in 28 cases (64%) of the CD group and 3 cases of (25%) the MD group (p=0.02). The mean hospital stay of the CD group was 21.5±15.9 days and that of the MD group was 41.4±29.4 days (p=0.04).
The predisposing factors of mediastinal extension in DNI were older age, involvement of two or more spaces, especially including the retropharyngeal space, and more comorbidities. The MD group had a longer hospital stay, higher mortality, and more failure to identify causative organisms of causative organisms than the CD group.
颈部深部感染(DNI)可源于颈部潜在间隙和筋膜平面的感染。DNI可不通过手术进行治疗,但有些病例需要手术治疗,尤其是在累及纵隔的情况下。本研究的目的是确定DNI的临床特征并分析纵隔扩展的易感因素。
我们回顾了2003年8月至2009年5月期间56例仅接受颈部引流的DNI患者(CD组)和因下行性坏死性纵隔炎接受颈部引流联合纵隔引流的患者(MD组)的病历,并比较了每组的临床特征和纵隔扩展的易感因素。
56例患者中有44例仅接受了颈部引流(79%),12例患者需要颈部和纵隔引流(21%)。两组在性别上无差异(p = 0.28),但MD组比CD组年龄更大(CD组,44.2±23.2岁;MD组,55.6±12.1岁;p = 0.03)。MD组合并症发生率高于CD组(p = 0.04)。CD组14例(32%)累及两个以上间隙,12例(27%)累及咽后间隙。MD组11例(92%)累及两个以上间隙,12例(100%)累及咽后间隙。CD组28例(64%)进行了病原体鉴定,MD组3例(25%)进行了病原体鉴定(p = 0.02)。CD组平均住院时间为21.5±15.9天,MD组为41.4±29.4天(p = 0.04)。
DNI纵隔扩展的易感因素包括年龄较大、累及两个或更多间隙,尤其是包括咽后间隙,以及更多的合并症。MD组比CD组住院时间更长、死亡率更高,且病原体鉴定失败的情况更多。