Sicras-Mainar Antoni, Velasco-Velasco Soledad, Navarro-Artieda Ruth, Prados-Torres Alexandra, Bolibar-Ribas Buenaventura, Violan-Fors Concepción
Directorate of Planning, Badalona Serveis Assistencials SA, Badalona, Barcelona, Spain.
BMJ Open. 2012 Jun 25;2(3). doi: 10.1136/bmjopen-2012-000941. Print 2012.
To describe the adaptive capacity of the Adjusted Clinical Groups (ACG) system to the cost of care in primary healthcare centres in Catalonia (Spain).
Retrospective study (multicentres) conducted using computerised medical records.
13 primary care teams in 2008 were included.
All patients registered in the study centres who required care between 1 January and 31 December 2008 were finally studied. Patients not registered in the study centres during the study period were excluded.
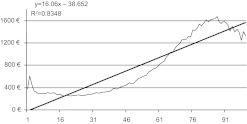
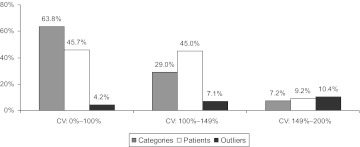
Demographic (age and sex), dependent (cost of care) and case-mix variables were studied. The cost model for each patient was established by differentiating the fixed and variable costs. To evaluate the adaptive capacity of the ACG system, Pearson's coefficient of variation and the percentage of outliers were calculated. To evaluate the explanatory power of the ACG system, the authors used the coefficient of determination (R(2)).
The number of patients studied was 227 235 (frequency: 5.9 visits per person per year), with a mean of 4.5 (3.2) episodes and 8.1 (8.2) visits per patient per year. The mean total cost was €654.2. The explanatory power of the ACG system was 36.9% for costs (56.5% without outliers). 10 ACG categories accounted for 60.1% of all cases and 19 for 80.9%. 5 categories represented 71% of poor performance (N=78 887, 34.7%), particularly category 0300-Acute Minor, Age 6+ (N=26 909, 11.8%), which had a coefficient of variation =139% and 6.6% of outliers.
The ACG system is an appropriate manner of classifying patients in routine clinical practice in primary healthcare centres in Catalonia, although improvements to the adaptive capacity through disaggregation of some categories according to age groups and, especially, the number of acute episodes in paediatric patients would be necessary to reduce intra-group variation.
描述调整后的临床分组(ACG)系统对加泰罗尼亚(西班牙)初级医疗中心护理成本的适应能力。
使用计算机化医疗记录进行的回顾性(多中心)研究。
纳入了2008年的13个初级保健团队。
最终研究了2008年1月1日至12月31日期间在研究中心登记且需要护理的所有患者。排除在研究期间未在研究中心登记的患者。
研究了人口统计学(年龄和性别)、相关指标(护理成本)和病例组合变量。通过区分固定成本和可变成本为每位患者建立成本模型。为评估ACG系统的适应能力,计算了Pearson变异系数和异常值百分比。为评估ACG系统的解释力,作者使用了决定系数(R²)。
研究的患者数量为227235人(频率:每人每年5.9次就诊),每位患者每年平均有4.5(3.2)次发作和8.1(8.2)次就诊。平均总成本为654.2欧元。ACG系统对成本的解释力为36.9%(无异常值时为56.5%)。10个ACG类别占所有病例的60.1%,19个占80.9%。5个类别占表现不佳病例的71%(N = 78887,34.7%),特别是0300 - 急性轻症,6岁及以上(N = 26909,11.8%),其变异系数 = 139%,异常值占6.6%。
ACG系统是加泰罗尼亚初级医疗中心常规临床实践中对患者进行分类的一种合适方式,尽管有必要通过根据年龄组对某些类别进行细分,尤其是儿科患者的急性发作次数,来提高适应能力,以减少组内变异。