Service de Chirurgie Maxillofaciale et Plastique, CHU Caen, France.
Acta Otorhinolaryngol Ital. 2012 Jun;32(3):145-53.
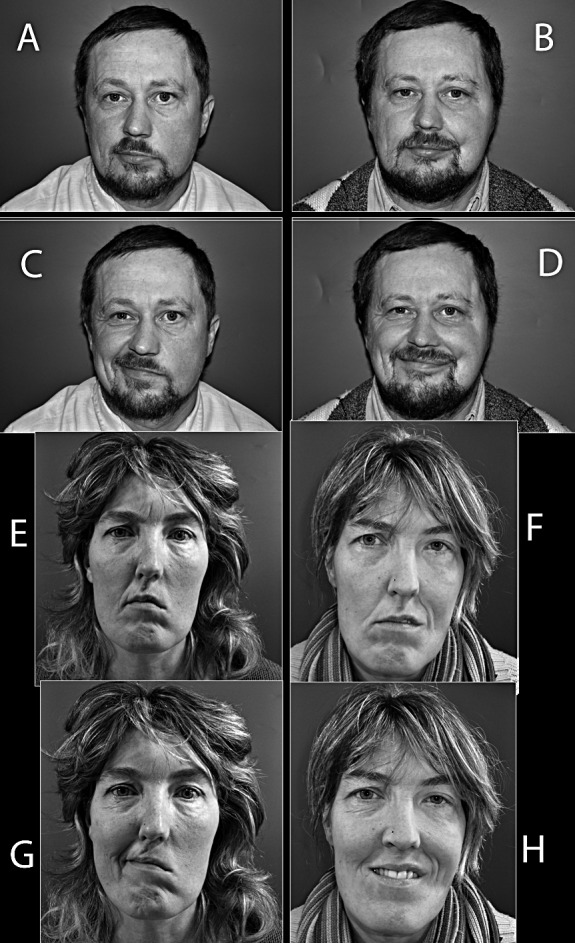
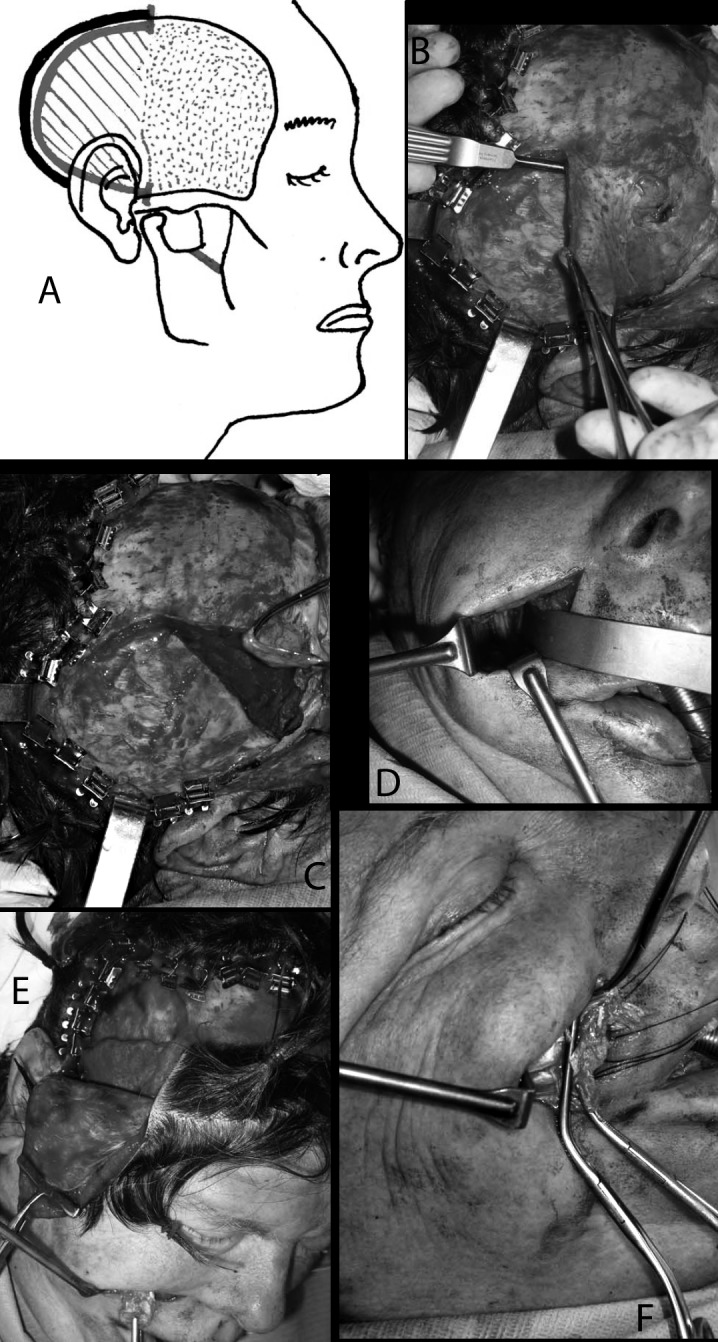
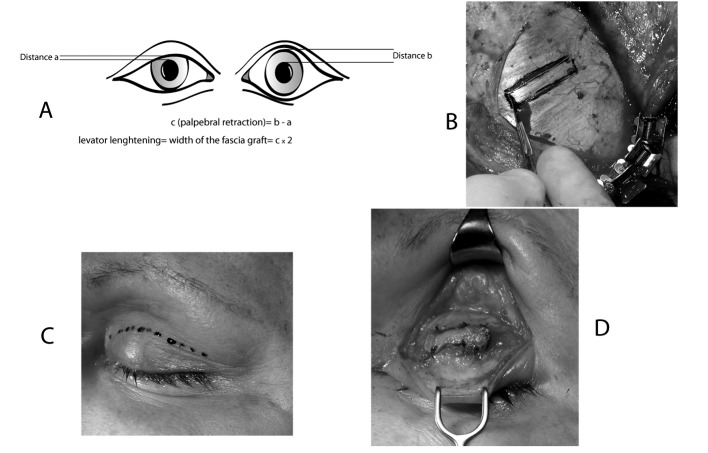
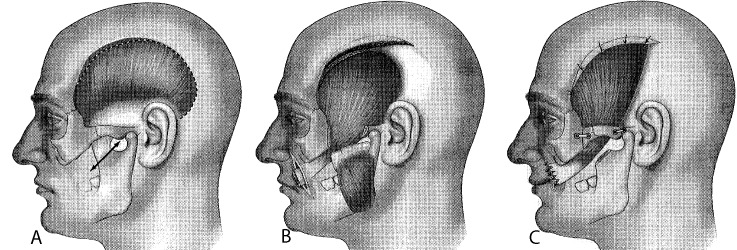
Long-standing peripheral monolateral facial paralysis in the adult has challenged otolaryngologists, neurologists and plastic surgeons for centuries. Notwithstanding, the ultimate goal of normality of the paralyzed hemi-face with symmetry at rest, and the achievement of a spontaneous symmetrical smile with corneal protection, has not been fully reached. At the beginning of the 20(th) century, the main options were neural reconstructions including accessory to facial nerve transfer and hypoglossal to facial nerve crossover. In the first half of the 20(th) century, various techniques for static correction with autologous temporalis muscle and fascia grafts were proposed as the techniques of Gillies (1934) and McLaughlin (1949). Cross-facial nerve grafts have been performed since the beginning of the 1970s often with the attempt to transplant free-muscle to restore active movements. However, these transplants were non-vascularized, and further evaluations revealed central fibrosis and minimal return of function. A major step was taken in the second half of the 1970s, with the introduction of microneurovascular muscle transfer in facial reanimation, which, often combined in two steps with a cross-facial nerve graft, has become the most popular option for the comprehensive treatment of long-standing facial paralysis. In the second half of the 1990s in France, a regional muscle transfer technique with the definite advantages of being one-step, technically easier and relatively fast, namely lengthening temporalis myoplasty, acquired popularity and consensus among surgeons treating facial paralysis. A total of 111 patients with facial paralysis were treated in Caen between 1997 and 2005 by a single surgeon who developed 2 variants of the technique (V1, V2), each with its advantages and disadvantages, but both based on the same anatomo-functional background and aim, which is transfer of the temporalis muscle tendon on the coronoid process to the lips. For a comprehensive treatment of the paralysis, the eyelids are usually managed by Paul Tessier's technique to lengthen the levator muscle of the upper eyelid by aponeurosis interposition, combined with external blepharorrhaphy with Krastinova-Lolov's technique. Facial reanimation using lengthening temporalis myoplasty is a dynamic procedure that has its roots in the techniques of Gillies and McLaughlin. This method is a true lengthening myoplasty procedure using no intermediate grafts. In general, the results with a 1-stage combination of lengthening temporalis myoplasty and static correction of the lagophthalmos appear comparable with the major series in the literature using free microneurovascular transfers combined with cross-facial nerve grafts for longstanding peripheral monolateral facial paralysis. The obvious advantages of temporalis elongation myoplasty consist in its technical ease, a single step, low incidence of complications and markedly reduced operating time.
成人长期单侧周围性面瘫数百年来一直困扰着耳鼻喉科医生、神经科医生和整形外科医生。尽管如此,使瘫痪半侧面部恢复正常,达到静止时对称,以及实现自发对称微笑和角膜保护的最终目标尚未完全实现。20 世纪初,主要的选择是包括副神经到面神经转移和舌下神经到面神经交叉的神经重建。在 20 世纪上半叶,各种采用自体胸锁乳突肌和筋膜移植物进行静态矫正的技术被提出,如吉尔(Gillies)(1934 年)和麦克劳克林(McLaughlin)(1949 年)的技术。自 20 世纪 70 年代初以来,人们一直在进行面-面神经移植,试图移植游离肌肉来恢复主动运动。然而,这些移植是非血管化的,进一步的评估显示中心纤维化和功能恢复最小。20 世纪 70 年代下半叶,面肌神经微血管转移在面部再神经化中的应用取得了重大进展,通常与面-面神经移植相结合分两步进行,已成为治疗长期面瘫的综合治疗的最受欢迎的选择。在 20 世纪 90 年代下半叶,法国的一种区域肌肉转移技术因其一步法、技术上更容易和相对较快的优势而获得普及和共识,即延长颞肌肌成形术,该技术由一位外科医生治疗面瘫患者,开发了两种技术(V1、V2),每种技术都有其优点和缺点,但都基于相同的解剖-功能背景和目标,即通过将颞肌肌腱转移到喙突来转移颞肌。为了对面瘫进行全面治疗,通常通过 Paul Tessier 的技术通过腱膜间置来延长上睑提肌,结合 Krastinova-Lolov 的技术进行外部睑成形术来治疗眼睑。使用延长颞肌肌成形术的面部再神经化是一种动态手术,其起源于吉尔和麦克劳克林的技术。这种方法是一种真正的延长肌成形术,不使用中间移植物。一般来说,在 1 期延长颞肌肌成形术和静态矫正下睑闭合不全的联合治疗中,使用文献中结合面-面神经移植的游离微血管神经转移治疗长期单侧周围性面瘫的主要系列结果具有可比性。延长颞肌肌成形术的明显优势在于其技术简单、一步法、并发症发生率低、手术时间明显缩短。