Schulich School of Medicine and Dentistry, The University of Western Ontario, 1151 Richmond Street, London, ON, Canada.
BMC Med Inform Decis Mak. 2012 Jul 7;12:63. doi: 10.1186/1472-6947-12-63.
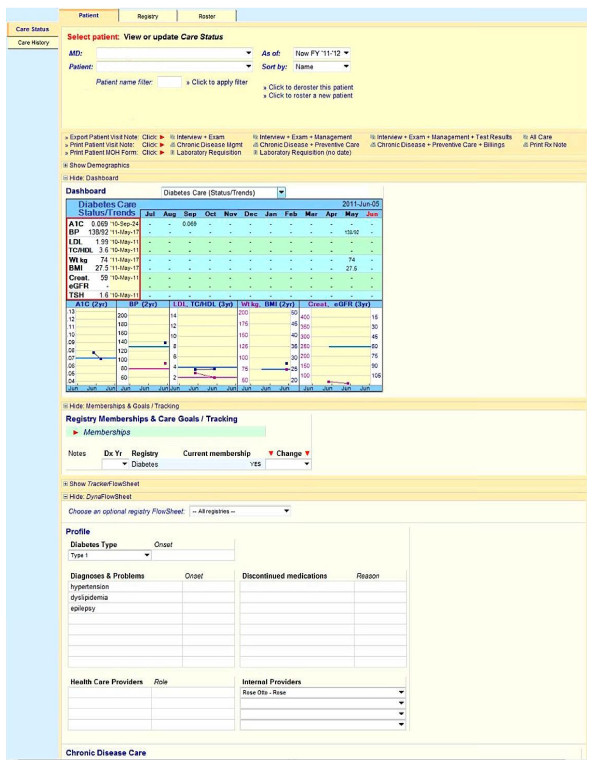
Physicians practicing in ambulatory care are adopting electronic health record (EHR) systems. Governments promote this adoption with financial incentives, some hinged on improvements in care. These systems can improve care but most demonstrations of successful systems come from a few highly computerized academic environments. Those findings may not be generalizable to typical ambulatory settings, where evidence of success is largely anecdotal, with little or no use of rigorous methods. The purpose of our pilot study was to evaluate the impact of a diabetes specific chronic disease management system (CDMS) on recording of information pertinent to guideline-concordant diabetes care and to plan for larger, more conclusive studies.
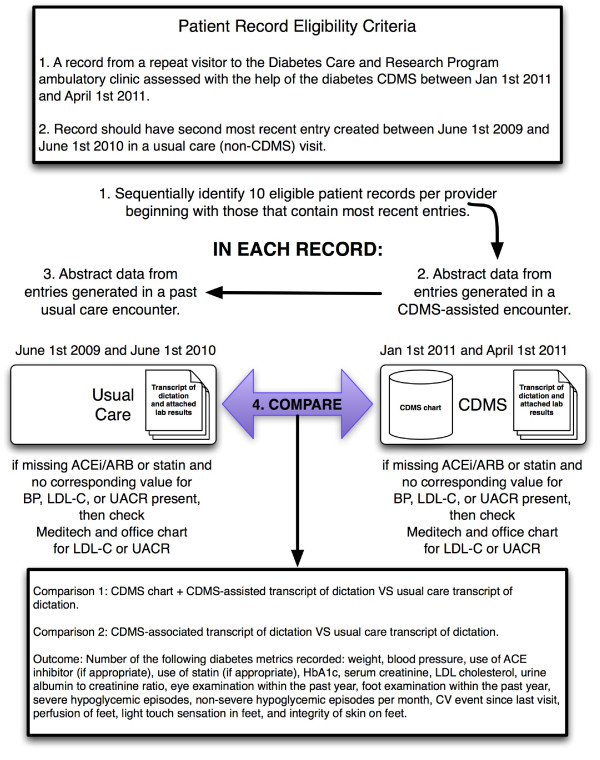
Using a before-after study design we analyzed the medical record of approximately 10 patients from each of 3 diabetes specialists (total = 31) who were seen both before and after the implementation of a CDMS. We used a checklist of key clinical data to compare the completeness of information recorded in the CDMS record to both the clinical note sent to the primary care physician based on that same encounter and the clinical note sent to the primary care physician based on the visit that occurred prior to the implementation of the CDMS, accounting for provider effects with Generalized Estimating Equations.
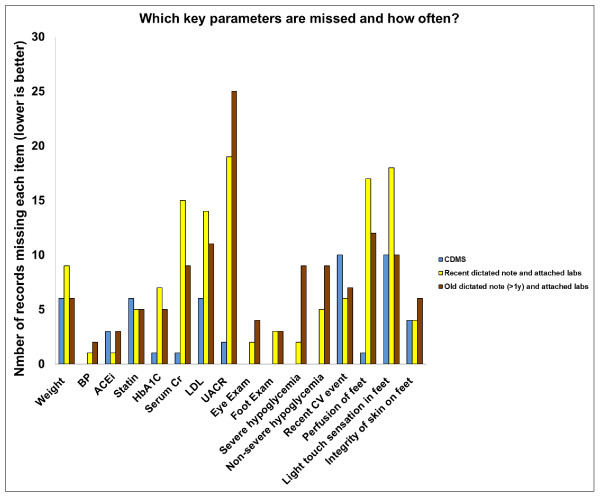
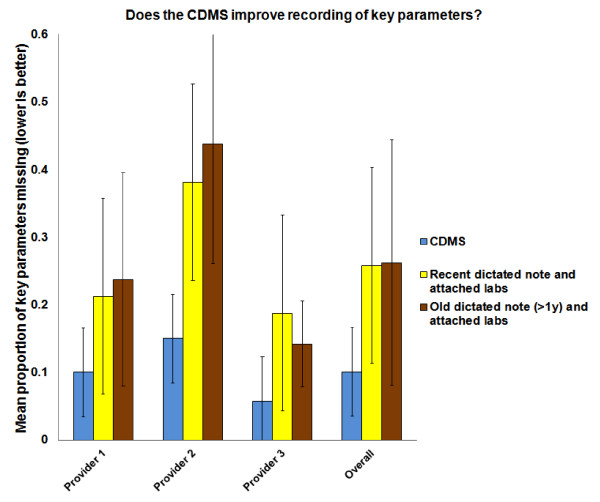
The CDMS record outperformed by a substantial margin dictated notes created for the same encounter. Only 10.1% (95% CI, 7.7% to 12.3%) of the clinically important data were missing from the CDMS chart compared to 25.8% (95% CI, 20.5% to 31.1%) from the clinical note prepared at the time (p < 0.001) and 26.3% (95% CI, 19.5% to 33.0%) from the clinical note prepared before the CDMS was implemented (p < 0.001). There was no significant difference between dictated notes created for the CDMS-assisted encounter and those created for usual care encounters (absolute mean difference, 0.8%; 95% CI, -8.5% to 6.8%).
The CDMS chart captured information important for the management of diabetes more often than dictated notes created with or without its use but we were unable to detect a difference in completeness between notes dictated in CDMS-associated and usual-care encounters. Our sample of patients and providers was small, and completeness of records may not reflect quality of care.
在门诊护理中执业的医生正在采用电子健康记录(EHR)系统。政府通过财政激励措施来促进这种采用,其中一些措施取决于护理质量的提高。这些系统可以改善护理,但大多数成功系统的证明都来自少数高度计算机化的学术环境。这些发现可能不适用于典型的门诊环境,在这些环境中,成功的证据主要是轶事,很少或根本没有使用严格的方法。我们的试点研究的目的是评估一个特定于糖尿病的慢性病管理系统(CDMS)对记录符合指南的糖尿病护理相关信息的影响,并为更大、更具结论性的研究做计划。
我们使用前后研究设计,分析了 3 名糖尿病专家(共 31 名)中每位患者大约 10 名患者的医疗记录,这些患者在实施 CDMS 前后都接受了治疗。我们使用关键临床数据检查表来比较 CDMS 记录中记录的信息的完整性与基于同一就诊情况发送给初级保健医生的临床记录以及基于实施 CDMS 之前就诊情况发送给初级保健医生的临床记录,使用广义估计方程来解释提供者的影响。
CDMS 记录的表现远远优于为同一就诊情况创建的记录。与当时准备的临床记录(p < 0.001)和实施 CDMS 之前准备的临床记录(p < 0.001)相比,CDMS 图表中仅缺少 10.1%(95%CI,7.7%至 12.3%)的临床重要数据,而记录中缺少 25.8%(95%CI,20.5%至 31.1%)和 26.3%(95%CI,19.5%至 33.0%)。在为 CDMS 辅助就诊创建的记录和为常规就诊创建的记录之间,记录的完整性没有显著差异(绝对平均差异,0.8%;95%CI,-8.5%至 6.8%)。
与没有使用 CDMS 或没有使用 CDMS 时创建的记录相比,CDMS 图表更经常记录对糖尿病管理很重要的信息,但我们未能检测到在与 CDMS 相关的就诊和常规就诊中记录的完整性之间的差异。我们的患者和提供者样本较小,记录的完整性可能并不能反映护理质量。