Carrara Alessandro, Mangiola Daniela, Pertile Riccardo, Ricci Alberta, Motter Michele, Ghezzi Gianmarco, Zappalà Orazio, Ciaghi Gianni, Tirone Giuseppe
1st Division of General Surgery, S. Chiara Hospital, 38122 Trento, Italy.
Int J Surg Oncol. 2012;2012:438450. doi: 10.1155/2012/438450. Epub 2012 Jun 19.
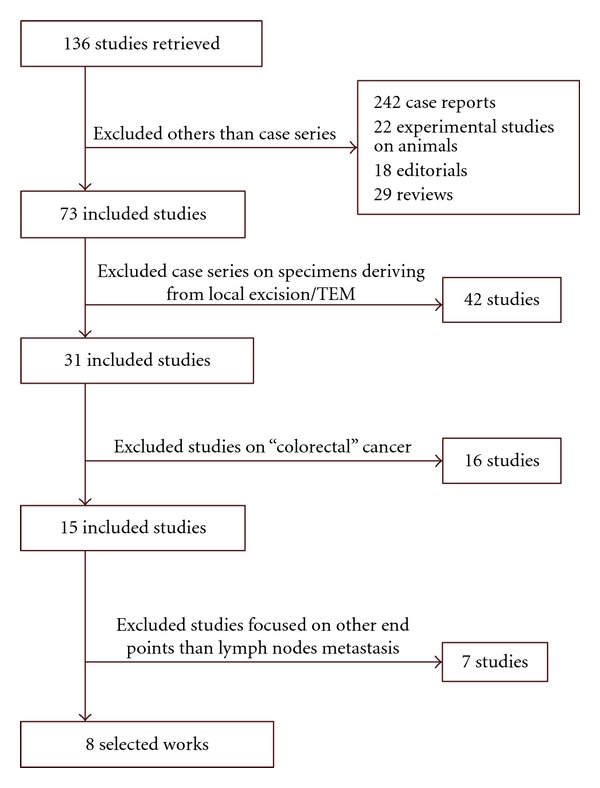
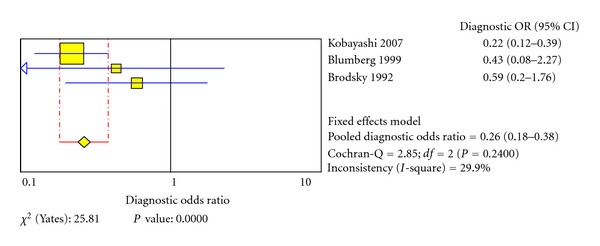
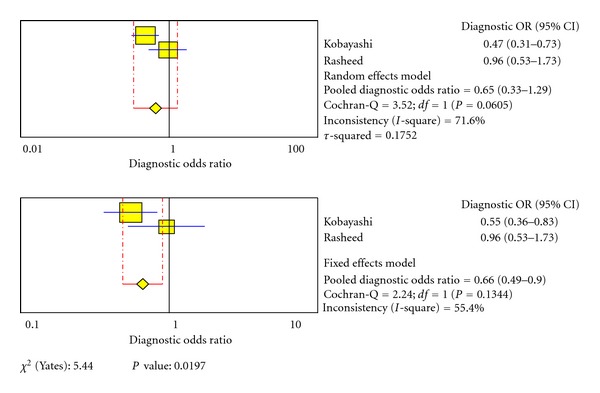
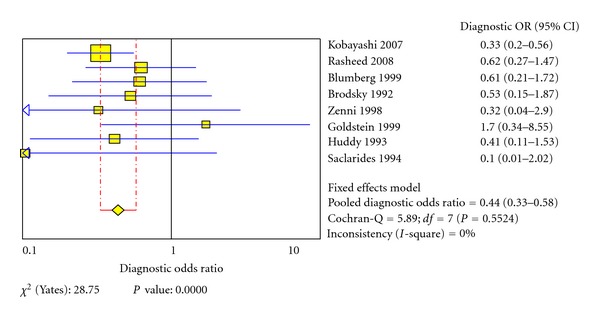
Background. Over the past ten years oncological outcomes achieved by local excision techniques (LETs) as the sole treatment for early stages of rectal cancer (ESRC) have been often disappointing. The reasons for these poor results lie mostly in the high risk of the disease's diffusion to local-regional lymph nodes even in ESRC. Aims. This study aims to find the correct indications for LET in ESRC taking into consideration clinical-pathological features of tumours that may reduce the risk of lymph node metastasis to zero. Methods. Systematic literature review and meta-analysis of casistics of ESRC treated with total mesorectal excision with the aim of identifying risk factors for nodal involvement. Results. The risk of lymph node metastasis is higher in G ≥ 2 and T ≥ 2 tumours with lymphatic and/or vascular invasion. Other features which have not yet been sufficiently investigated include female gender, TSM stage >1, presence of tumour budding and/or perineural invasion. Conclusions. Results comparable to radical surgery can be achieved by LET only in patients with T(1) N(0) G(1) tumours with low-risk histological features, whereas deeper or more aggressive tumours should be addressed by radical surgery (RS).
背景。在过去十年中,局部切除技术(LETs)作为早期直肠癌(ESRC)的唯一治疗方法所取得的肿瘤学结果常常令人失望。这些不良结果的原因主要在于,即使是在ESRC中,疾病扩散至局部区域淋巴结的风险也很高。目的。本研究旨在考虑可能将淋巴结转移风险降至零的肿瘤临床病理特征,找出ESRC中LET的正确适应证。方法。对接受全直肠系膜切除术治疗的ESRC病例进行系统文献回顾和荟萃分析,以确定淋巴结受累的危险因素。结果。在G≥2和T≥2且伴有淋巴管和/或血管侵犯的肿瘤中,淋巴结转移风险更高。其他尚未得到充分研究的特征包括女性性别、TSM分期>1、肿瘤出芽和/或神经周围侵犯。结论。仅在具有低风险组织学特征的T(1)N(0)G(1)肿瘤患者中,LET才能取得与根治性手术相当的结果,而对于更深或更具侵袭性的肿瘤,则应采用根治性手术(RS)。