JAMA. 2012 Jun 20;307(23):2499-506. doi: 10.1001/jama.2012.6571.
The value of assessing various emerging lipid-related markers for prediction of first cardiovascular events is debated.
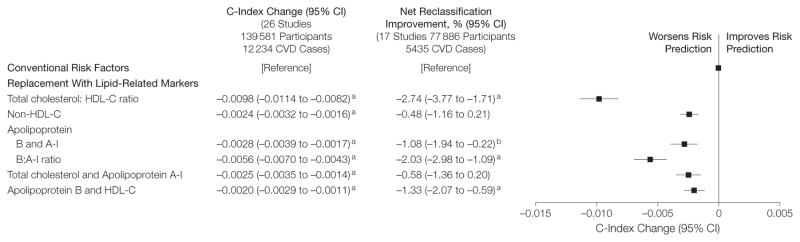
To determine whether adding information on apolipoprotein B and apolipoprotein A-I, lipoprotein(a), or lipoprotein-associated phospholipase A2 to total cholesterol and high-density lipoprotein cholesterol (HDL-C) improves cardiovascular disease (CVD) risk prediction.
DESIGN, SETTING, AND PARTICIPANTS: Individual records were available for 165,544 participants without baseline CVD in 37 prospective cohorts (calendar years of recruitment: 1968-2007) with up to 15,126 incident fatal or nonfatal CVD outcomes (10,132 CHD and 4994 stroke outcomes) during a median follow-up of 10.4 years (interquartile range, 7.6-14 years).
Discrimination of CVD outcomes and reclassification of participants across predicted 10-year risk categories of low (<10%), intermediate (10%-<20%), and high (≥20%) risk.
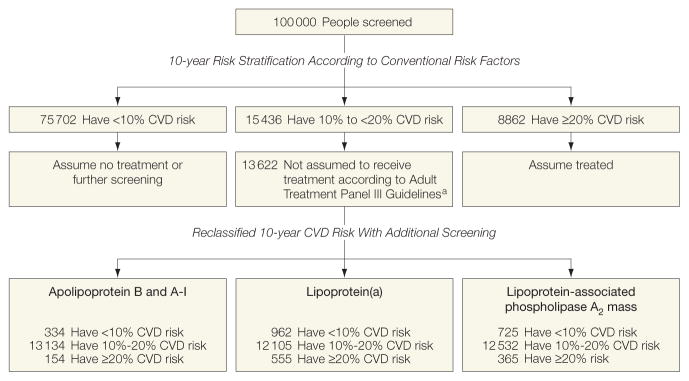
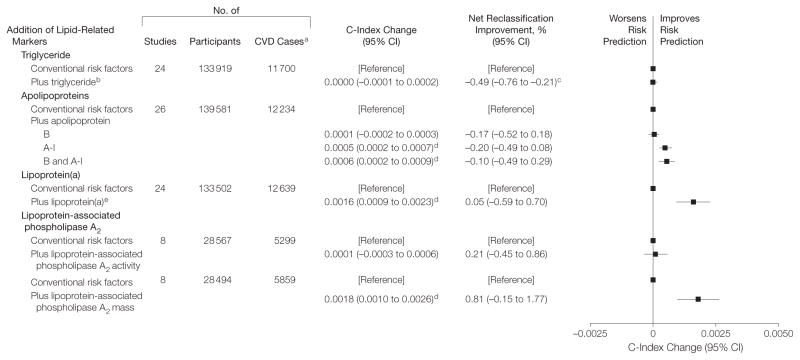
The addition of information on various lipid-related markers to total cholesterol, HDL-C, and other conventional risk factors yielded improvement in the model's discrimination: C-index change, 0.0006 (95% CI, 0.0002-0.0009) for the combination of apolipoprotein B and A-I; 0.0016 (95% CI, 0.0009-0.0023) for lipoprotein(a); and 0.0018 (95% CI, 0.0010-0.0026) for lipoprotein-associated phospholipase A2 mass. Net reclassification improvements were less than 1% with the addition of each of these markers to risk scores containing conventional risk factors. We estimated that for 100,000 adults aged 40 years or older, 15,436 would be initially classified at intermediate risk using conventional risk factors alone. Additional testing with a combination of apolipoprotein B and A-I would reclassify 1.1%; lipoprotein(a), 4.1%; and lipoprotein-associated phospholipase A2 mass, 2.7% of people to a 20% or higher predicted CVD risk category and, therefore, in need of statin treatment under Adult Treatment Panel III guidelines.
In a study of individuals without known CVD, the addition of information on the combination of apolipoprotein B and A-I, lipoprotein(a), or lipoprotein-associated phospholipase A2 mass to risk scores containing total cholesterol and HDL-C led to slight improvement in CVD prediction.
评估各种新兴的与脂质相关的标志物在预测首发心血管事件中的价值存在争议。
确定在总胆固醇和高密度脂蛋白胆固醇(HDL-C)中添加载脂蛋白 B 和载脂蛋白 A-I、脂蛋白(a)或脂蛋白相关磷脂酶 A2 的信息是否能改善心血管疾病(CVD)风险预测。
设计、地点和参与者:37 项前瞻性队列研究(招募年份:1968-2007 年)中共有 165544 名基线无 CVD 的参与者的个体记录,中位随访 10.4 年(四分位间距,7.6-14 年)期间发生了 15126 例致死性或非致死性 CVD 事件(10132 例 CHD 和 4994 例卒中等事件)。
对 CVD 结局的区分和将参与者按低(<10%)、中(10%-<20%)和高(≥20%)风险预测 10 年风险类别重新分类。
将各种与脂质相关的标志物的信息添加到总胆固醇、HDL-C 和其他常规危险因素中,可提高模型的区分度:C 指数变化分别为载脂蛋白 B 和 A-I 组合为 0.0006(95%CI,0.0002-0.0009);脂蛋白(a)为 0.0016(95%CI,0.0009-0.0023);脂蛋白相关磷脂酶 A2 质量为 0.0018(95%CI,0.0010-0.0026)。将这些标志物中的每一个添加到包含常规危险因素的风险评分中,净重新分类改善均小于 1%。我们估计,对于 100000 名年龄在 40 岁或以上的成年人,单独使用常规危险因素,有 15436 人最初被归类为中危人群。使用载脂蛋白 B 和 A-I 的联合检测,将有 1.1%的人重新归类为 20%或更高的 CVD 风险预测类别,因此需要根据成人治疗小组 III 指南接受他汀类药物治疗;脂蛋白(a)为 4.1%;脂蛋白相关磷脂酶 A2 质量为 2.7%。
在一项无已知 CVD 的个体研究中,在包含总胆固醇和 HDL-C 的风险评分中添加载脂蛋白 B 和 A-I、脂蛋白(a)或脂蛋白相关磷脂酶 A2 质量的信息,可略微改善 CVD 预测。