Adamzik Michael, Hamburger Tim, Petrat Frank, Peters Jürgen, de Groot Herbert, Hartmann Matthias
Crit Care. 2012 Jul 16;16(4):R125. doi: 10.1186/cc11425.
Hemolysis can be induced in sepsis via various mechanisms, its pathophysiological importance has been demonstrated in experimental sepsis. However, no data on free hemoglobin concentrations in human sepsis are available. In the present study we measured free hemoglobin in patients with severe sepsis as well as in postoperative patients using four methods. It was our aim to determine the potential value of free hemoglobin as a biomarker for diagnosis and outcome of severe sepsis in critical illness.
Plasma concentration of free hemoglobin was determined in patients with severe sepsis (n = 161) and postoperative patients (n = 136) on day 1 of diagnosis and surgery. For the measurement of free hemoglobin, an enzyme linked immunosorbent assay and three spectrophotometric algorithms were used. Moreover, SAPS II- and SOFA scores as well as procalcitonin concentration and outcome were determined. Kaplan-Meier analysis was performed and odds ratios were determined after classification of free hemoglobin concentrations in a high and low concentration group according to the median. For statistical evaluation the Mann-Whitney test and logistic regression analysis were used.
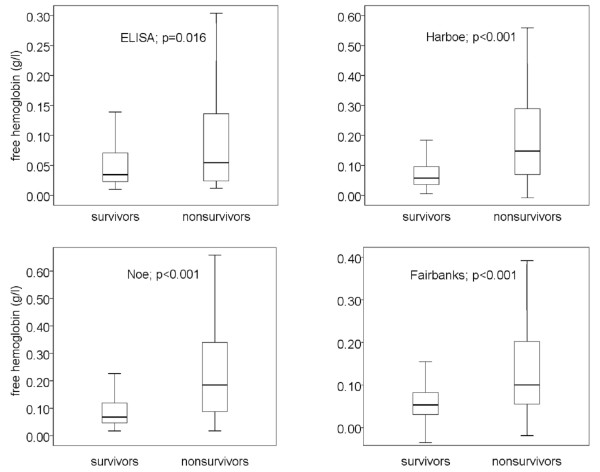
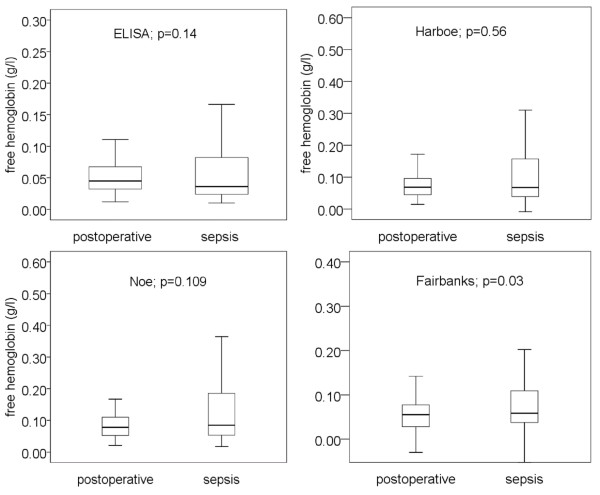
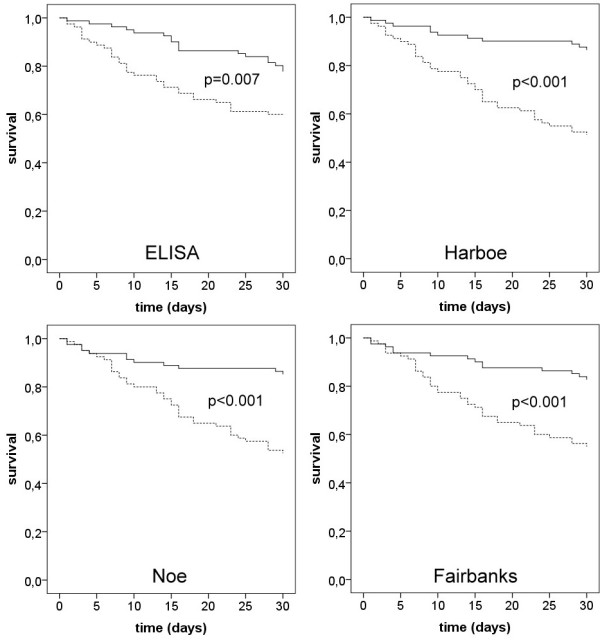
In non-survivors of severe sepsis, free hemoglobin concentration was twice the concentration compared to survivors. Thirty-day survival of patients, as evidenced by Kaplan-Meier analysis, was markedly lower in patients with high free hemoglobin concentration than in patients with low free hemoglobin concentration. Best discrimination of outcome was achieved with the spectrophotometric method of Harboe (51.3% vs. 86.4% survival, p < 0.001; odds ratio 6.1). Multivariate analysis including free hemoglobin, age, SAPS II- and SOFA-score and procalcitonin demonstrated that free hemoglobin, as determined by all 4 methods, was the best and an independent predictor for death in severe sepsis (p = 0.022 to p < 0.001). Free hemoglobin concentrations were not significantly different in postoperative and septic patients in three of four assays. Thus, free hemoglobin can not be used to diagnose severe sepsis in critical illness.
Free hemoglobin is an important new predictor of survival in severe sepsis.
脓毒症可通过多种机制诱发溶血,其病理生理重要性已在实验性脓毒症中得到证实。然而,目前尚无关于人类脓毒症中游离血红蛋白浓度的数据。在本研究中,我们使用四种方法测量了重症脓毒症患者以及术后患者的游离血红蛋白。我们的目的是确定游离血红蛋白作为危重症中重症脓毒症诊断和预后生物标志物的潜在价值。
在诊断和手术第1天,测定重症脓毒症患者(n = 161)和术后患者(n = 136)的血浆游离血红蛋白浓度。采用酶联免疫吸附测定法和三种分光光度法来测量游离血红蛋白。此外,还测定了序贯器官衰竭评估(SOFA)评分、简化急性生理学评分(SAPS II)以及降钙素原浓度和预后情况。进行Kaplan-Meier分析,并在根据中位数将游离血红蛋白浓度分为高浓度组和低浓度组后确定比值比。采用Mann-Whitney检验和逻辑回归分析进行统计学评估。
在重症脓毒症非幸存者中,游离血红蛋白浓度是幸存者的两倍。Kaplan-Meier分析表明,游离血红蛋白浓度高的患者30天生存率明显低于游离血红蛋白浓度低的患者。使用Harboe分光光度法对预后的区分效果最佳(生存率分别为51.3%和86.4%,p < 0.001;比值比为6.1)。包括游离血红蛋白、年龄、SAPS II评分、SOFA评分和降钙素原的多变量分析表明,通过所有4种方法测定的游离血红蛋白是重症脓毒症死亡的最佳且独立预测指标(p = 0.022至p < 0.001)。在四种检测方法中的三种中,术后患者和脓毒症患者的游离血红蛋白浓度无显著差异。因此,游离血红蛋白不能用于危重症中重症脓毒症的诊断。
游离血红蛋白是重症脓毒症生存的重要新预测指标。