Department of Nuclear Medicine and Molecular Imaging, University Medical Center Groningen, University of Groningen, PO Box 30.001, 9700 RB, Groningen, The Netherlands.
Eur J Nucl Med Mol Imaging. 2012 Oct;39(10):1609-17. doi: 10.1007/s00259-012-2187-8. Epub 2012 Jul 18.
Cardiac amyloidosis is a rare disorder, but it may lead to potentially life-threatening restrictive cardiomyopathy. Cardiac manifestations frequently occur in primary amyloidosis (AL) and familial amyloidosis (ATTR), but are uncommon in secondary amyloidosis (AA). Echocardiography is the method of choice for assessing cardiac amyloidosis. Amyloid deposits impair the function of sympathetic nerve endings. Disturbance of myocardial sympathetic innervations may play an important role in the remodelling process. (123)I-MIBG can detect these innervation changes.
Patients with biopsy-proven amyloidosis underwent general work-up, echocardiography and (123)I-MIBG scintigraphy. Left ventricular internal dimensions and wall thickness were measured, and highly refractile cardiac echoes (sparkling) were analysed. Early (15 min) and late (4 h) heart-to-mediastinum ratio (HMR) and wash-out rate were determined after administration of MIBG.
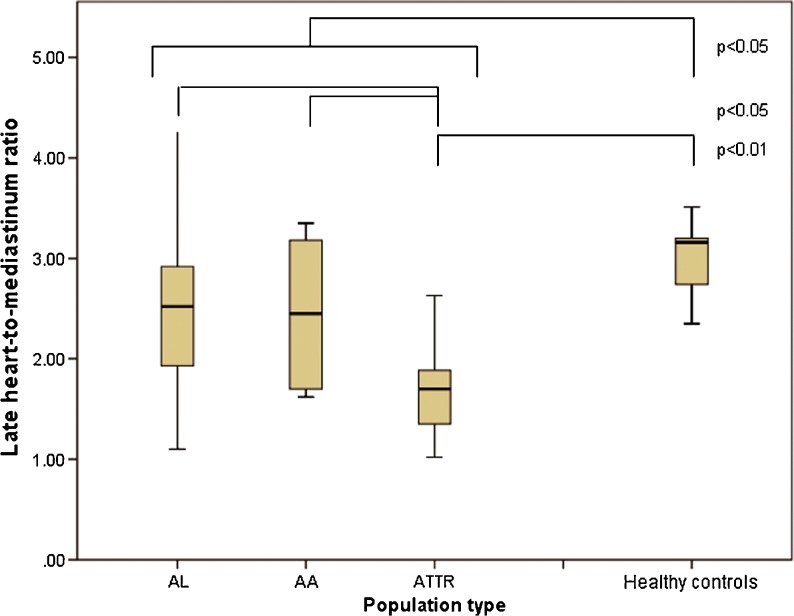
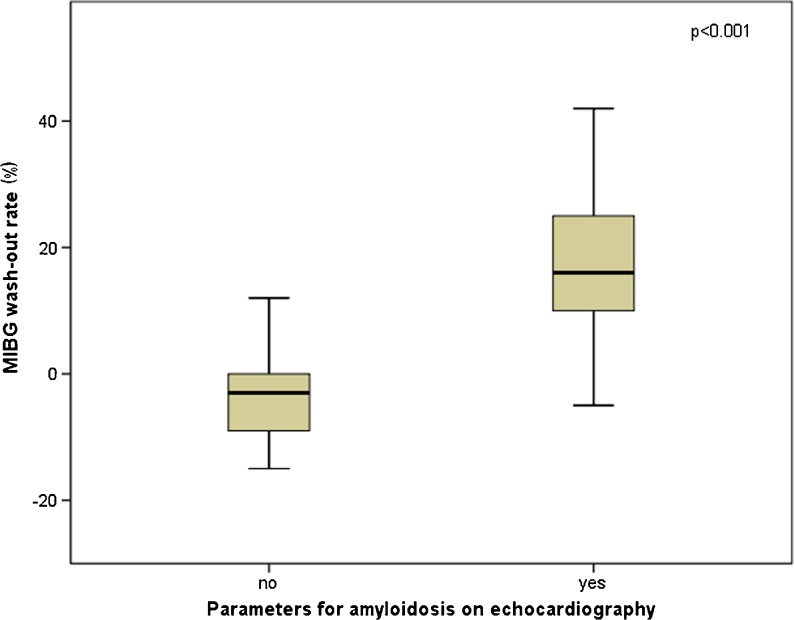
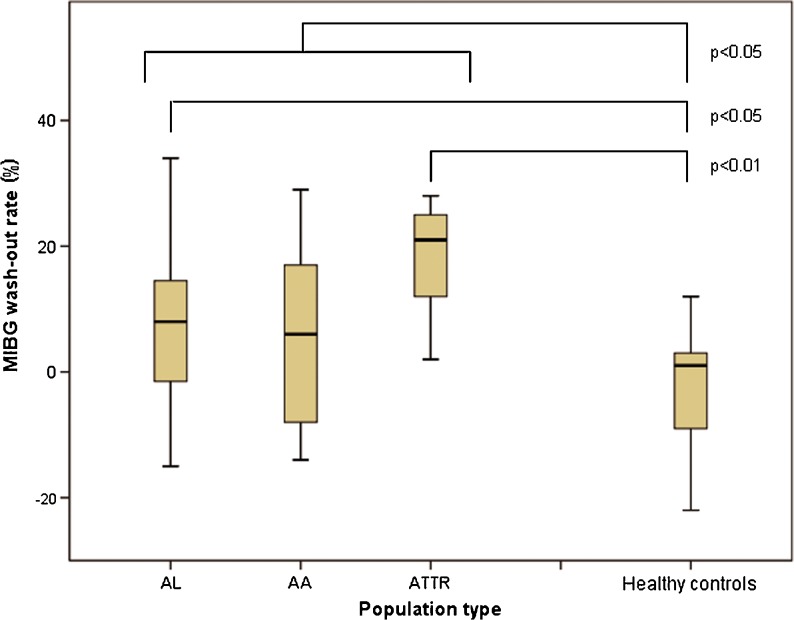
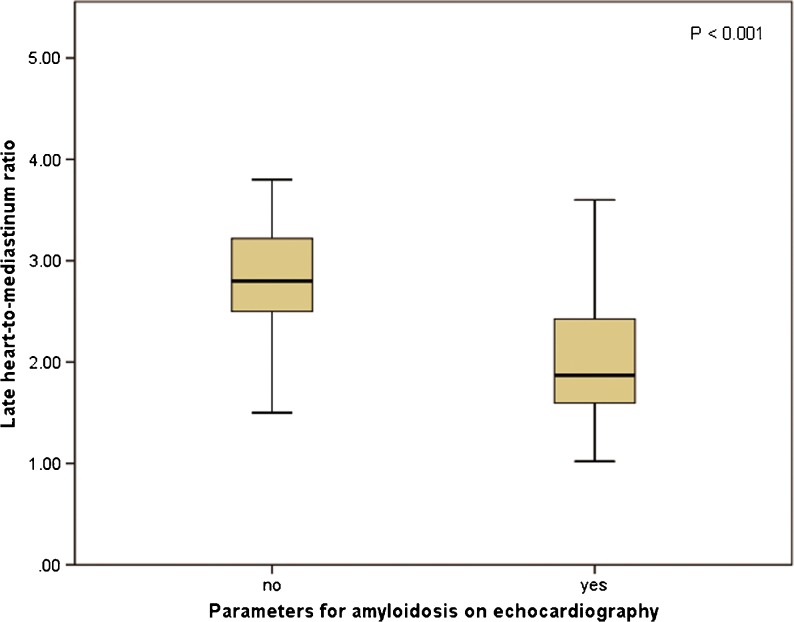
Included in the study were 61 patients (30 women and 31 men; mean age 62 years; 39 AL, 11 AA, 11 ATTR). Echocardiographic parameters were not significantly different between the groups. Sparkling was present in 72 % of ATTR patients, in 54 % of AL patients and in 45 % of AA patients. Mean late HMR in all patients was 2.3 ± 0.75, and the mean wash-out rate was 8.6 ± 14 % (the latter not significantly different between the patient groups). Late HMR was significantly lower in patients with echocardiographic signs of amyloidosis than in patients without (2.0 ± 0.70 versus 2.8 ± 0.58, p < 0.001). Wash-out rates were significantly higher in these patients (-3.3 ± 9.9 % vs. 17 ± 10 %, p < 0.001). In ATTR patients without echocardiographic signs of amyloidosis, HMR was lower than in patients with the other types (2.0 ± 0.59 vs. 2.9 ± 0.50, p = 0.007).
MIBG HMR is lower and wash-out rate is higher in patients with echocardiographic signs of amyloidosis. Also, (123)I-MIBG scintigraphy can detect cardiac denervation in ATTR patients before signs of amyloidosis are evident on echocardiography.
心脏淀粉样变性是一种罕见的疾病,但它可能导致潜在危及生命的限制性心肌病。心脏表现常发生在原发性淀粉样变性(AL)和家族性淀粉样变性(ATTR)中,但在继发性淀粉样变性(AA)中并不常见。超声心动图是评估心脏淀粉样变性的首选方法。淀粉样沉积物会损害交感神经末梢的功能。心肌交感神经支配的紊乱可能在重塑过程中发挥重要作用。(123)I-MIBG 可检测到这些神经支配的变化。
经活检证实为淀粉样变性的患者接受了全面检查、超声心动图和(123)I-MIBG 闪烁显像。测量左心室内部尺寸和壁厚度,并分析高度反光的心脏回声(闪烁)。在 MIBG 给药后 15 分钟(早期)和 4 小时(晚期)测定心脏与纵隔的比值(HMR)和洗脱率。
本研究共纳入 61 例患者(30 名女性和 31 名男性;平均年龄 62 岁;39 例 AL、11 例 AA、11 例 ATTR)。各组间超声心动图参数无显著差异。72%的 ATTR 患者、54%的 AL 患者和 45%的 AA 患者存在闪烁现象。所有患者的平均晚期 HMR 为 2.3±0.75,洗脱率为 8.6±14%(各组间无显著差异)。有超声心动图淀粉样变性征象的患者的晚期 HMR 明显低于无淀粉样变性征象的患者(2.0±0.70 与 2.8±0.58,p<0.001)。这些患者的洗脱率明显较高(-3.3±9.9%与 17±10%,p<0.001)。在无超声心动图淀粉样变性征象的 ATTR 患者中,HMR 低于其他类型的患者(2.0±0.59 与 2.9±0.50,p=0.007)。
有超声心动图淀粉样变性征象的患者,(123)I-MIBG HMR 较低,洗脱率较高。此外,(123)I-MIBG 闪烁显像术可在超声心动图显示淀粉样变性前检测到 ATTR 患者的心脏去神经支配。