Modeling & Simulation, Novartis Institutes for Biomedical Research, 45 Sidney St, Cambridge, MA, USA.
BMC Cancer. 2012 Jul 23;12:311. doi: 10.1186/1471-2407-12-311.
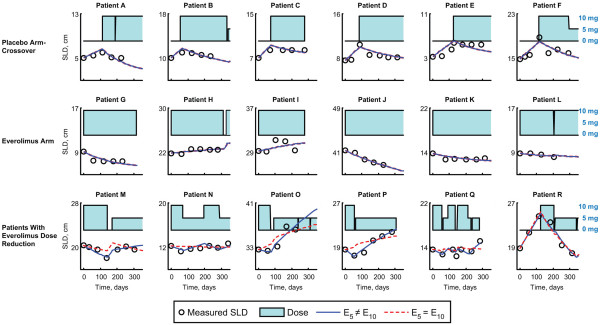
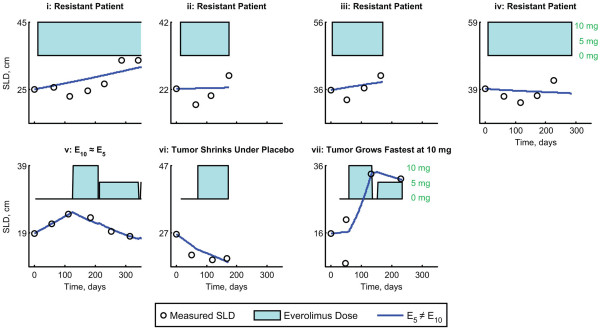
The phase 3 RECORD-1 trial (NCT00410124) established the efficacy and safety of everolimus in patients with metastatic renal cell carcinoma (mRCC) who progress on sunitinib or sorafenib. In RECORD-1, patients received 10 mg everolimus daily, with dose reduction to 5 mg daily allowed for toxicity. We have developed a model of tumor growth dynamics utilizing serial measurements of the sum of the longest tumor diameters (SLD) from individual RECORD-1 patients to define the dose-response relationship of everolimus.
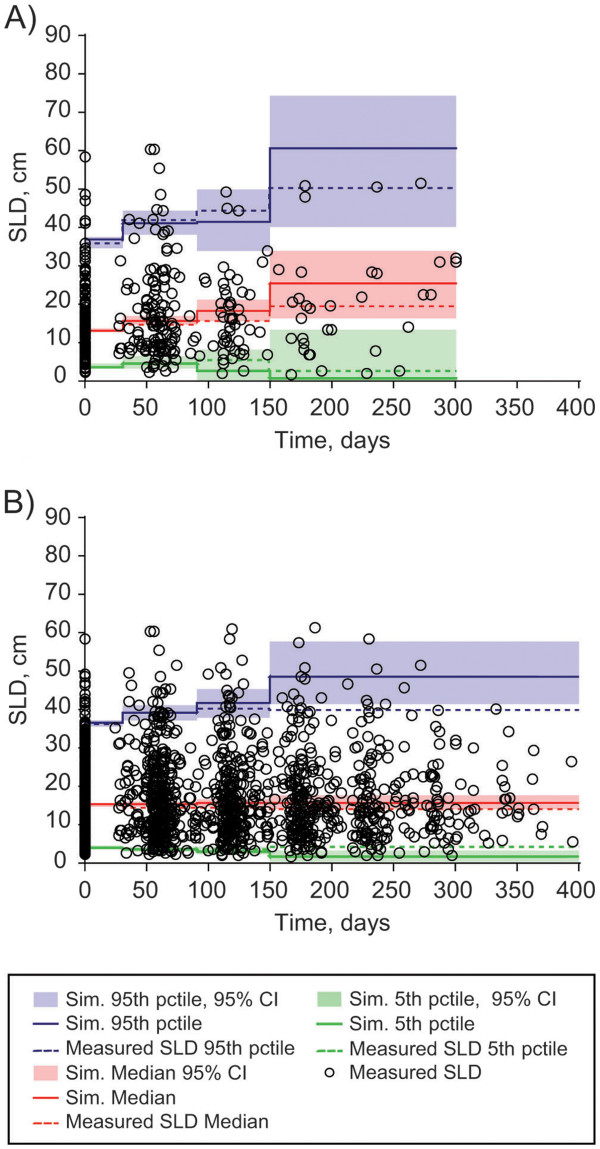
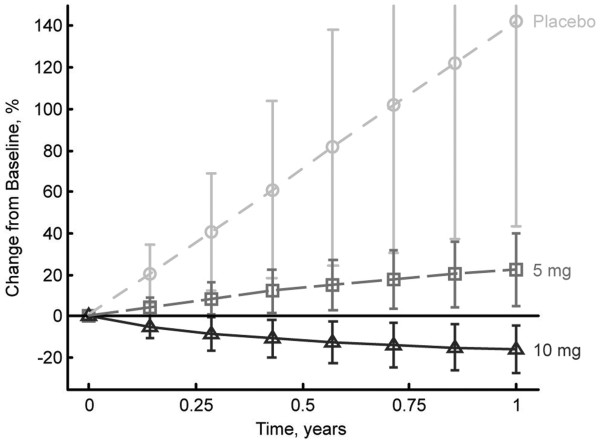
The model predicts that after 1 year of continuous dosing, the change in SLD of target lesions will be +142.1% ± 98.3%, +22.4% ± 17.2%, and -15.7% ± 11.5% in the average patient treated with placebo, 5 mg everolimus, and 10 mg everolimus, respectively. This nonlinear, mixed-effects modeling approach can be used to describe the dynamics of each individual patient, as well as the overall population. This allows evaluation of how an actual dosing history and individual covariates impact on the observed drug effect, and offers the possibility of predicting clinical observations as a function of time.
In this pharmacodynamic model of tumor response, everolimus more effectively shrinks target lesions in mRCC when dosed 10 mg daily versus 5 mg daily, although a 5-mg dose still shows an antitumor effect. These data support earlier studies that established 10 mg daily as the preferred clinical dose of everolimus, and improve our understanding of the everolimus dose-response relationship.
RECORD-1 期临床试验(NCT00410124)确立了依维莫司在索拉非尼或舒尼替尼治疗后进展的转移性肾细胞癌(mRCC)患者中的疗效和安全性。在 RECORD-1 中,患者每天接受 10mg 依维莫司治疗,毒性允许剂量减少至 5mg 每天。我们利用 RECORD-1 中个别患者最长肿瘤直径总和(SLD)的连续测量值开发了一种肿瘤生长动力学模型,以确定依维莫司的剂量反应关系。
该模型预测,在持续治疗 1 年后,接受安慰剂、5mg 依维莫司和 10mg 依维莫司治疗的平均患者的目标病变 SLD 变化将分别为+142.1%±98.3%、+22.4%±17.2%和-15.7%±11.5%。这种非线性混合效应建模方法可用于描述每个个体患者以及总体人群的动力学。这允许评估实际给药历史和个体协变量如何影响观察到的药物作用,并提供了根据时间预测临床观察的可能性。
在这种肿瘤反应的药效动力学模型中,与每天 5mg 相比,每天 10mg 依维莫司更有效地缩小 mRCC 中的目标病变,尽管 5mg 剂量仍显示出抗肿瘤作用。这些数据支持了较早的研究,该研究确立了每天 10mg 作为依维莫司的首选临床剂量,并提高了我们对依维莫司剂量反应关系的理解。