Respiratory Institute, Cleveland, Ohio, USA.
Pulm Circ. 2012 Apr-Jun;2(2):220-8. doi: 10.4103/2045-8932.97609.
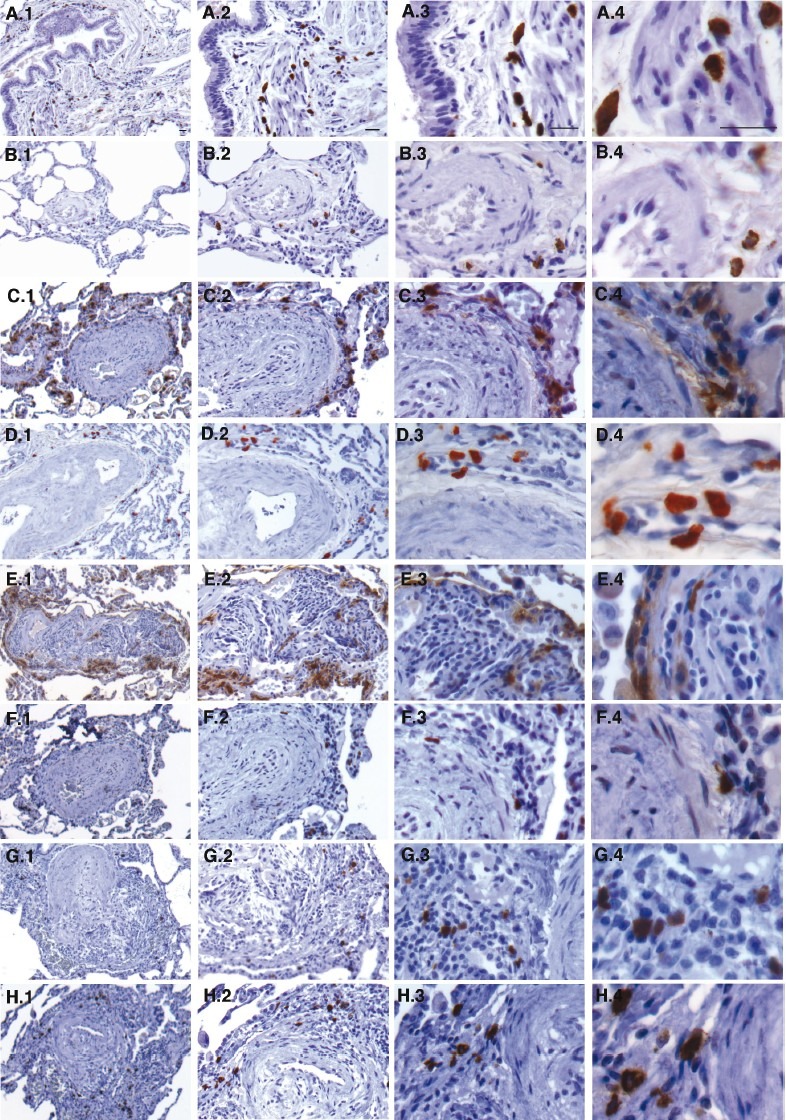
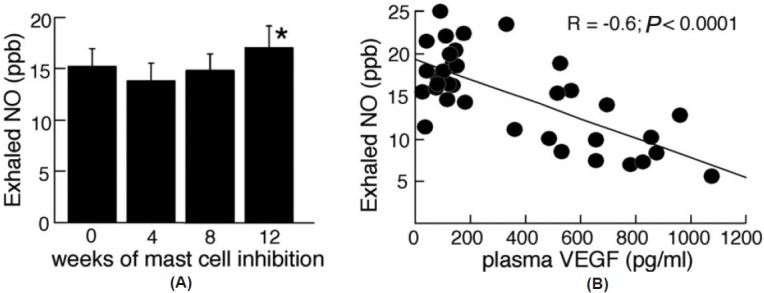
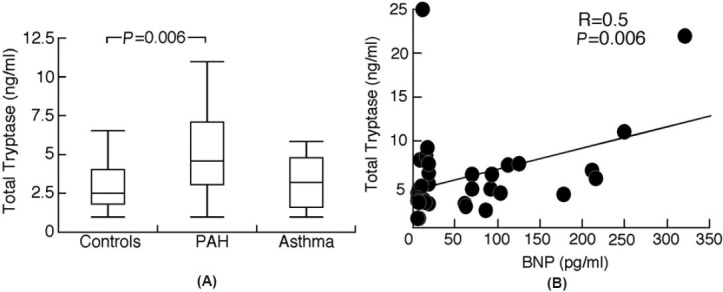
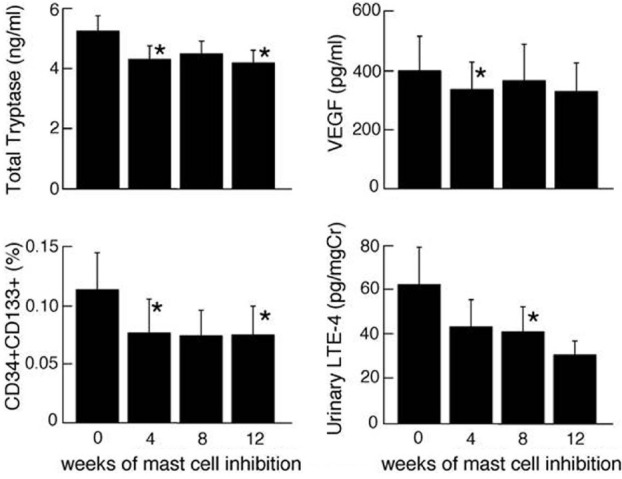
A proliferation of mast cells around the small pulmonary blood vessels and the alveolar septae has been noted in models of pulmonary hypertension, and in plexiform lesions of pulmonary arterial hypertension (PAH) in patients. Here, we hypothesize that total mast cell numbers and activation are increased in PAH and that they contribute to vascular remodeling through cellular and soluble proangiogenic effectors. To test this, blood and urine were collected from patients with PAH (N=44), asthma (N=18) and healthy controls (N=29) to quantitate biomarkers of total body mast cell numbers and activation (total and mature tryptase, N-methyl histamine, leukotriene LTE(4) and prostaglandin PGD-M). Serum total tryptase was higher in PAH than that in controls suggesting greater numbers of mast cells, but indicators of mast cell activation (mature tryptase, LTE(4) and PGD-M) were similar among PAH, asthma, and controls. Immunohistochemistry of lung tissues identified mast cells as primarily perivascular and connective tissue chymase(+) type in PAH, rather than mucosal phenotype. Intervention with mast cell inhibitors cromolyn and fexofenadine was performed in 9 patients for 12 weeks to identify the influence of mast cell products on the pathologic proangiogenic environment. Treatment decreased total tryptase and LTE-4 levels over time of treatment. This occurred in parallel to a drop in vascular endothelial growth factor (VEGF) and circulating proangiogenic CD34+CD133+ progenitor cells, which suggests that mast cells may promote vascular remodeling and dysfunction. In support of this, levels of exhaled nitric oxide, a vasodilator that is generally low in PAH, increased at the end of the 12-week mast cell blockade and antihistamine. These results suggest that mast cells might contribute to the pulmonary vascular pathologic processes underlying PAH. More studies are needed to confirm their potential contribution to the disease.
在肺动脉高压的模型中以及在肺动脉高压(PAH)患者的复杂病变中,已经注意到肺小血管周围和肺泡隔中的肥大细胞增殖。在这里,我们假设 PAH 中的总肥大细胞数量和激活增加,并且它们通过细胞和可溶性促血管生成效应物促进血管重塑。为了验证这一点,从 PAH 患者(N=44)、哮喘患者(N=18)和健康对照者(N=29)中收集血液和尿液,以定量测定全身肥大细胞数量和激活的生物标志物(总和成熟的胰蛋白酶、N-甲基组氨酸、白三烯 LTE(4)和前列腺素 PGD-M)。PAH 患者的血清总胰蛋白酶高于对照组,表明肥大细胞数量更多,但肥大细胞激活的指标(成熟胰蛋白酶、LTE(4)和 PGD-M)在 PAH、哮喘和对照组之间相似。肺组织的免疫组织化学鉴定出肥大细胞在 PAH 中主要是血管周围和结缔组织糜蛋白酶(+)型,而不是粘膜表型。对 9 例患者进行了 12 周的肥大细胞抑制剂 cromolyn 和 fexofenadine 干预,以确定肥大细胞产物对病理性促血管生成环境的影响。随着治疗时间的延长,治疗会降低总胰蛋白酶和 LTE-4 水平。这与血管内皮生长因子(VEGF)和循环促血管生成 CD34+CD133+祖细胞的下降同时发生,这表明肥大细胞可能促进血管重塑和功能障碍。支持这一点的是,一氧化氮呼气的水平增加,通常在 PAH 中较低,在 12 周的肥大细胞阻断和抗组胺治疗结束时增加。这些结果表明,肥大细胞可能有助于 PAH 下的肺血管病理过程。需要更多的研究来证实它们对疾病的潜在贡献。