Columbia University College of Physicians and Surgeons, New York, NY, USA.
J Thorac Cardiovasc Surg. 2013 Aug;146(2):296-301. doi: 10.1016/j.jtcvs.2012.07.020. Epub 2012 Jul 28.
Vasoactive medications improve hemodynamics after cardiac surgery but are associated with high metabolic and arrhythmic burdens. The vasoactive-inotropic score was developed to quantify vasoactive and inotropic support after cardiac surgery in pediatric patients but may be useful in adults as well. Accordingly, we examined the time course of this score in a substudy of the Biventricular Pacing After Cardiac Surgery trial. We hypothesized that the score would be lower in patients randomized to biventricular pacing.
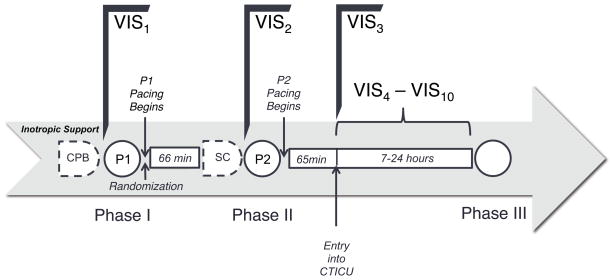
Fifty patients selected for increased risk of left ventricular dysfunction after cardiac surgery and randomized to temporary biventricular pacing or standard of care (no pacing) after cardiopulmonary bypass were studied in a clinical trial between April 2007 and June 2011. Vasoactive agents were assessed after cardiopulmonary bypass, after sternal closure, and 0 to 7 hours after admission to the intensive care unit.
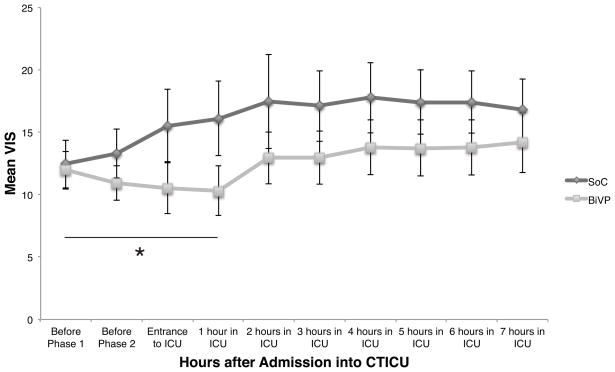
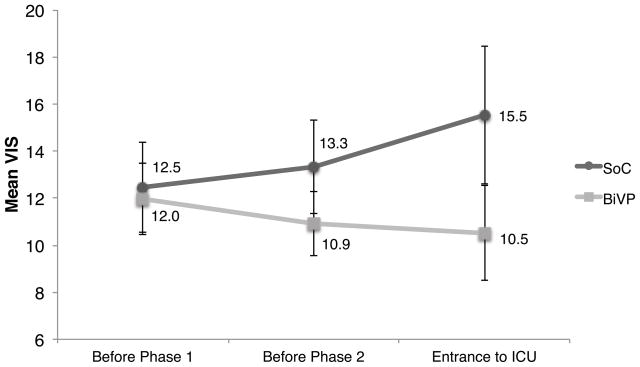
Over the initial 3 collection points after cardiopulmonary bypass (mean duration, 131 minutes), the mean vasoactive-inotropic score decreased in the biventricular pacing group from 12.0 ± 1.5 to 10.5 ± 2.0 and increased in the standard of care group from 12.5 ± 1.9 to 15.5 ± 2.9. By using a linear mixed-effects model, the slopes of the time courses were significantly different (P = .02) and remained so for the first hour in the intensive care unit. However, the difference was no longer significant beyond this point (P = .26).
The vasoactive-inotropic score decreases in patients undergoing temporary biventricular pacing in the early postoperative period. Future studies are required to assess the impact of this effect on arrhythmogenesis, morbidity, mortality, and hospital costs.
血管活性药物可改善心脏手术后的血液动力学,但与代谢和心律失常负担高有关。血管活性-正性肌力评分用于量化心脏手术后儿科患者的血管活性和正性肌力支持,但在成人中也可能有用。因此,我们在心脏手术后双心室起搏试验的子研究中检查了该评分的时间过程。我们假设该评分在随机接受双心室起搏的患者中较低。
在 2007 年 4 月至 2011 年 6 月期间进行的一项临床试验中,选择了 50 名患者进行心脏手术后左心室功能障碍风险增加,并随机分配接受体外循环后临时双心室起搏或标准治疗(无起搏)。在体外循环后、胸骨关闭后和入住重症监护病房 0 至 7 小时时评估血管活性药物。
在体外循环后最初的 3 个采集点(平均持续时间 131 分钟),双心室起搏组的血管活性-正性肌力评分从 12.0±1.5 降至 10.5±2.0,标准治疗组从 12.5±1.9 增至 15.5±2.9。使用线性混合效应模型,时间过程的斜率差异显著(P=0.02),在重症监护病房的前 1 小时内仍然如此。然而,在此之后,差异不再显著(P=0.26)。
在术后早期接受临时双心室起搏的患者中,血管活性-正性肌力评分降低。需要进一步研究来评估这种作用对心律失常发生、发病率、死亡率和医院成本的影响。