Duke Clinical Research Institute, Duke University Medical Center, Durham, NC 27710, USA.
JAMA. 2012 Aug 1;308(5):475-84. doi: 10.1001/jama.2012.8363.
The safety and durability of endoscopic vein graft harvest in coronary artery bypass graft (CABG) surgery has recently been called into question.
To compare the long-term outcomes of endoscopic vs open vein-graft harvesting for Medicare patients undergoing CABG surgery in the United States.
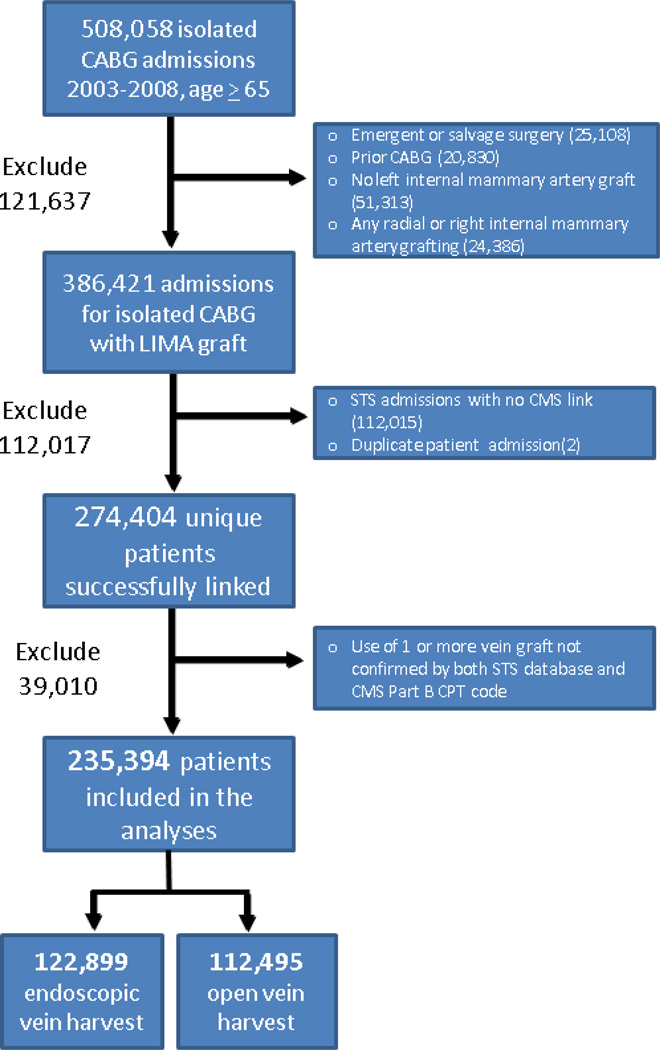
DESIGN, SETTING, AND PATIENTS: An observational study of 235,394 Medicare patients undergoing isolated CABG surgery between 2003 and 2008 at 934 surgical centers participating in the Society of Thoracic Surgeons (STS) national database. The STS records were linked to Medicare files to allow longitudinal assessment (median 3-year follow-up) through December 31, 2008.
All-cause mortality. Secondary outcome measures included wound complications and the composite of death, myocardial infarction, and revascularization.
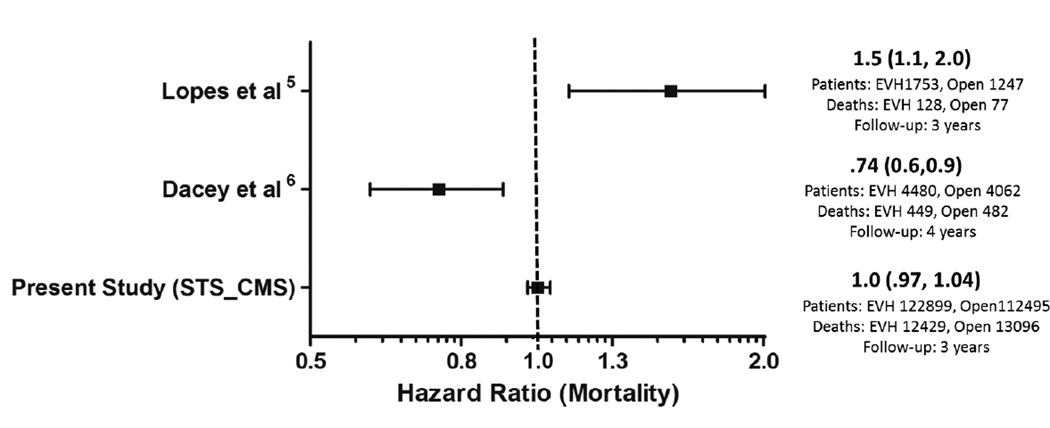
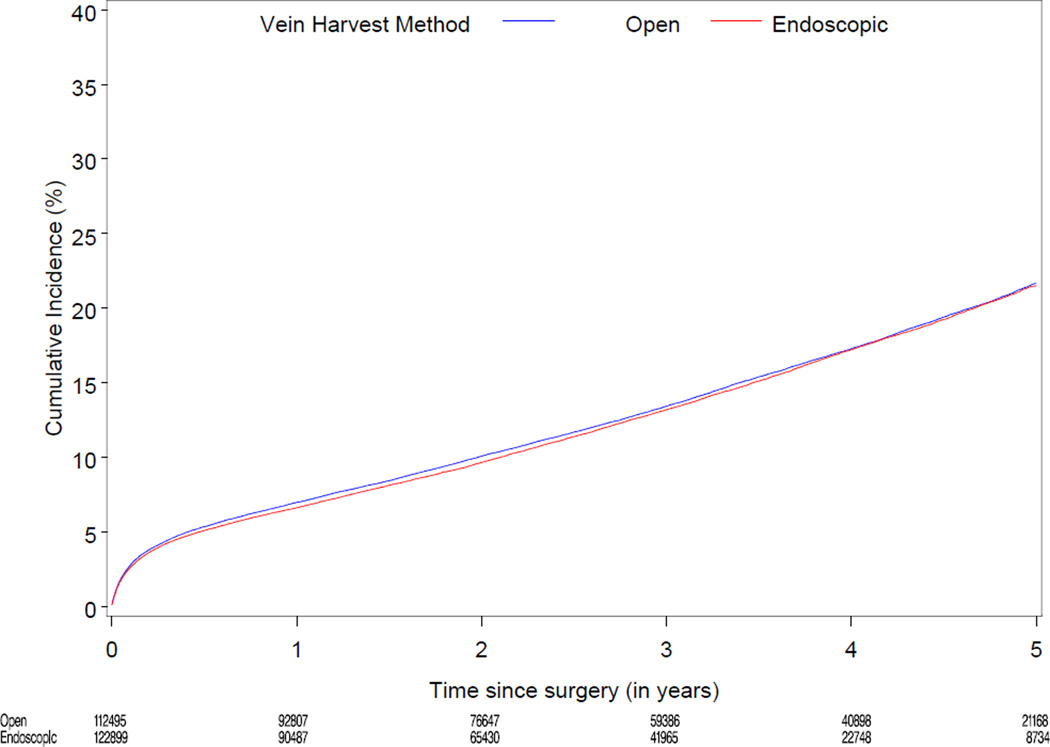
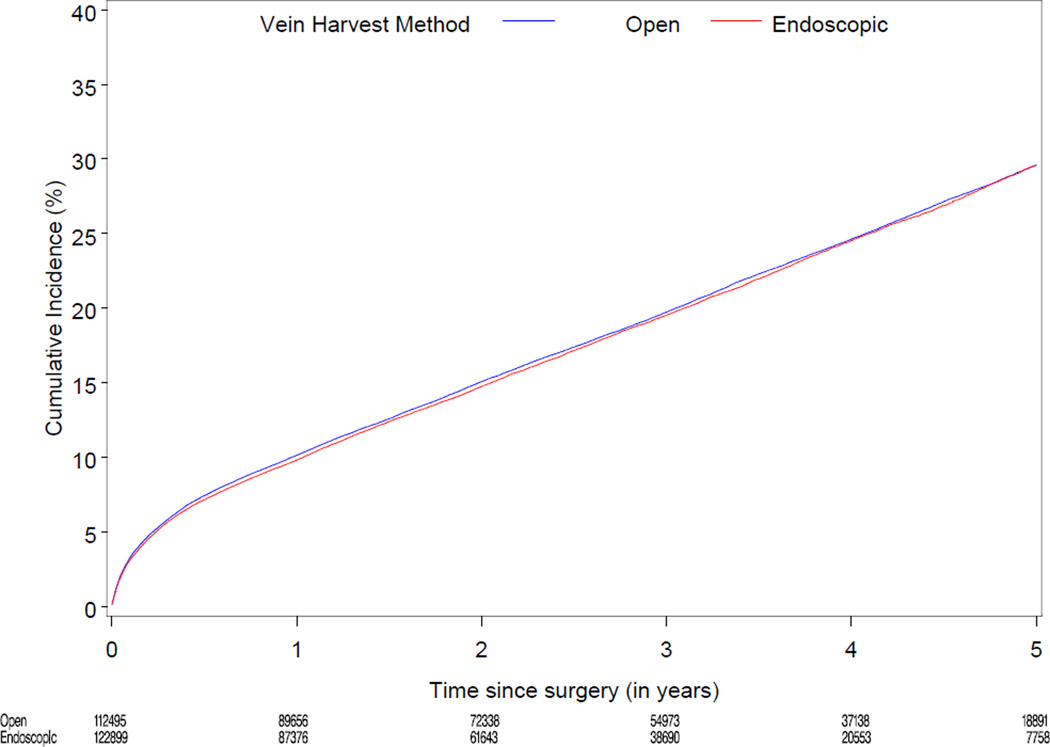
Based on Medicare Part B coding, 52% of patients received endoscopic vein-graft harvesting during CABG surgery. After propensity score adjustment for clinical characteristics, there were no significant differences between long-term mortality rates (13.2% [12,429 events] vs 13.4% [13,096 events]) and the composite of death, myocardial infarction, and revascularization (19.5% [18,419 events] vs 19.7% [19,232 events]). Time-to-event analysis for those patients receiving endoscopic vs open vein-graft harvesting revealed adjusted hazard ratios [HRs] of 1.00 (95% CI, 0.97-1.04) for mortality and 1.00 (95% CI, 0.98-1.05) for the composite outcome. Endoscopic vein-graft harvesting was associated with lower harvest site wound complications relative to open vein-graft harvesting (3.0% [3654/122,899 events] vs 3.6% [4047/112,495 events]; adjusted HR, 0.83; 95% CI, 0.77-0.89; P < .001).
Among patients undergoing CABG surgery, the use of endoscopic vein-graft harvesting compared with open vein-graft harvesting was not associated with increased mortality.
内镜下静脉采集用于冠状动脉旁路移植术(CABG)中的安全性和耐久性最近受到质疑。
比较美国医疗保险患者接受 CABG 手术时内镜与开放式静脉采集的长期结果。
设计、地点和患者:一项观察性研究,纳入 2003 年至 2008 年期间在参与胸外科医师学会(STS)国家数据库的 934 个外科中心接受单纯 CABG 手术的 235394 名医疗保险患者。STS 记录与医疗保险文件相关联,允许通过 2008 年 12 月 31 日进行纵向评估(中位数 3 年随访)。
全因死亡率。次要终点包括伤口并发症和死亡、心肌梗死和血运重建的复合终点。
根据医疗保险 B 部分编码,52%的患者在 CABG 手术中接受了内镜下静脉采集。在对临床特征进行倾向评分调整后,长期死亡率(13.2%[12,429 例事件]与 13.4%[13,096 例事件])和死亡、心肌梗死和血运重建的复合终点(19.5%[18,419 例事件]与 19.7%[19,232 例事件])之间无显著差异。对接受内镜下与开放式静脉采集的患者进行时间事件分析,显示死亡率的调整后危险比(HR)为 1.00(95%CI,0.97-1.04),复合终点的调整后 HR 为 1.00(95%CI,0.98-1.05)。与开放式静脉采集相比,内镜下静脉采集与较低的采集部位伤口并发症相关(3.0%[3654/122899 例事件]与 3.6%[4047/112495 例事件];调整后的 HR,0.83;95%CI,0.77-0.89;P<0.001)。
在接受 CABG 手术的患者中,与开放式静脉采集相比,使用内镜下静脉采集与死亡率增加无关。