Division of Human Nutrition, Department of Agricultural, Food & Nutritional Science, University of Alberta, Edmonton, Canada.
Br J Cancer. 2012 Sep 4;107(6):931-6. doi: 10.1038/bjc.2012.350. Epub 2012 Aug 7.
Skeletal muscle depletion (sarcopenia) predicts morbidity and mortality in the elderly and cancer patients.
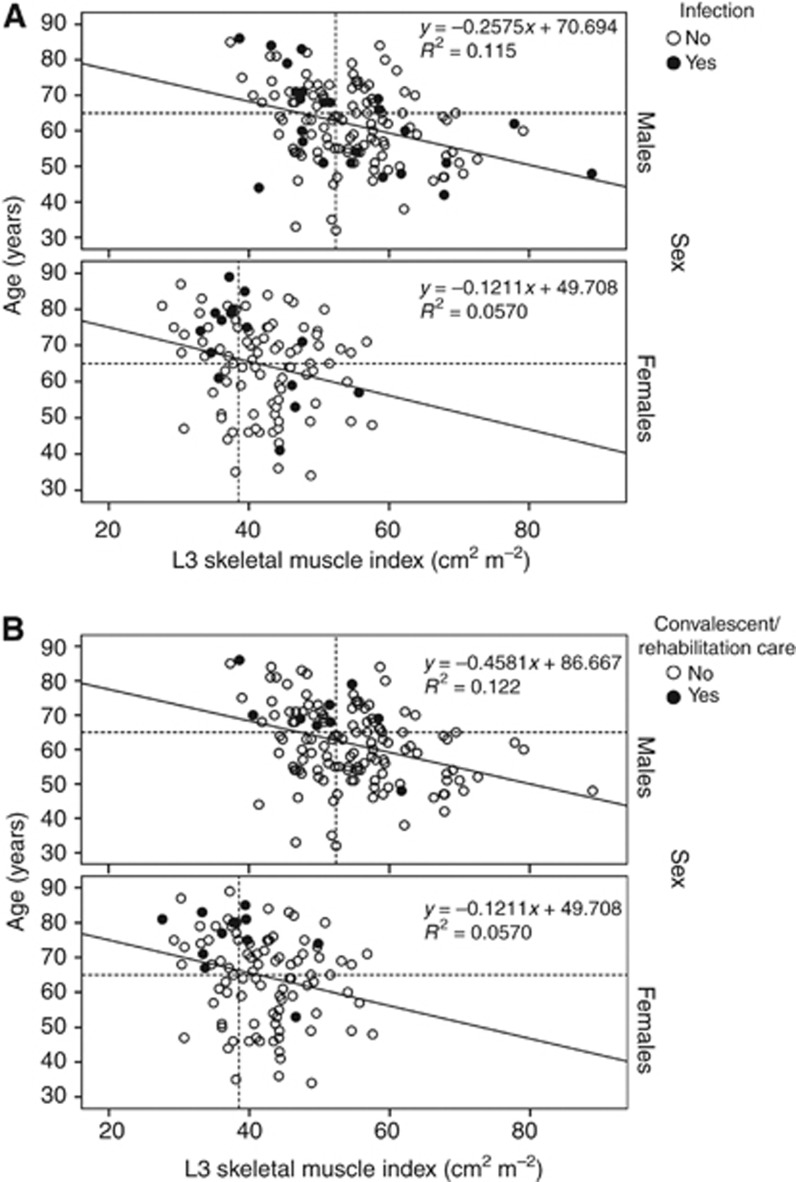
We tested whether sarcopenia predicts primary colorectal cancer resection outcomes in stage II-IV patients (n=234). Sarcopenia was assessed using preoperative computed tomography images. Administrative hospitalisation data encompassing the index surgical admission, direct transfers for inpatient rehabilitation care and hospital re-admissions within 30 days was searched for International Classification of Disease (ICD)-10 codes for postoperative infections and inpatient rehabilitation care and used to calculate length of stay (LOS).
Overall, 38.9% were sarcopenic; 16.7% had an infection and 9.0% had inpatient rehabilitation care. Length of stay was longer for sarcopenic patients overall (15.9 ± 14.2 days vs 12.3 ± 9.8 days, P=0.038) and especially in those ≥ 65 years (20.2 ± 16.9 days vs 13.1 ± 8.3 days, P=0.008). Infection risk was greater for sarcopenic patients overall (23.7% vs 12.5%; P=0.025), and especially those ≥ 65 years (29.6% vs 8.8%, P=0.005). Most (90%) inpatient rehabilitation care was in patients ≥ 65 years. Inpatient rehabilitation was more common in sarcopenic patients overall (14.3% vs 5.6%; P=0.024) and those ≥ 65 years (24.1% vs 10.7%, P=0.06). In a multivariate model in patients ≥ 65 years, sarcopenia was an independent predictor of both infection (odds ratio (OR) 4.6, (95% confidence interval (CI) 1.5, 13.9) P<0.01) and rehabilitation care (OR 3.1 (95% CI 1.04, 9.4) P<0.04).
Sarcopenia predicts postoperative infections, inpatient rehabilitation care and consequently a longer LOS.
骨骼肌减少(肌少症)可预测老年人和癌症患者的发病率和死亡率。
我们测试了肌少症是否可以预测 II-IV 期患者(n=234)的原发性结直肠癌切除术的结果。使用术前计算机断层扫描图像评估肌少症。搜索了国际疾病分类(ICD)-10 代码,以查找索引手术入院、直接转至住院康复护理以及 30 天内再次入院的术后感染和住院康复护理的行政住院数据,并用于计算住院时间(LOS)。
总体而言,38.9%的患者存在肌少症;16.7%的患者发生感染,9.0%的患者需要住院康复护理。肌少症患者的总体住院时间较长(15.9 ± 14.2 天 vs 12.3 ± 9.8 天,P=0.038),尤其是 65 岁以上的患者(20.2 ± 16.9 天 vs 13.1 ± 8.3 天,P=0.008)。总体而言,肌少症患者的感染风险更高(23.7% vs 12.5%;P=0.025),尤其是 65 岁以上的患者(29.6% vs 8.8%,P=0.005)。大多数(90%)住院康复护理患者年龄均在 65 岁以上。肌少症患者的住院康复护理更为常见(14.3% vs 5.6%;P=0.024),尤其是 65 岁以上的患者(24.1% vs 10.7%,P=0.06)。在 65 岁以上患者的多变量模型中,肌少症是感染(优势比(OR)4.6,(95%置信区间(CI)1.5,13.9)P<0.01)和康复护理(OR 3.1(95% CI 1.04,9.4)P<0.04)的独立预测因素。
肌少症可预测术后感染、住院康复护理以及因此导致的住院时间延长。