Intensive Care Unit, Hospital General Universitario Gregorio Marañón, Calle Doctor Esquerdo 46, Madrid, 28007, Spain.
Ann Intensive Care. 2012 Jul 5;2 Suppl 1(Suppl 1):S3. doi: 10.1186/2110-5820-2-S1-S3.
The aim of this study was to determine the incidence of intra-abdominal hypertension (IAH) in patients with two or more categorized risk factors (CRF) for IAH, and their morbidity and mortality during their intensive care unit (ICU) stay.
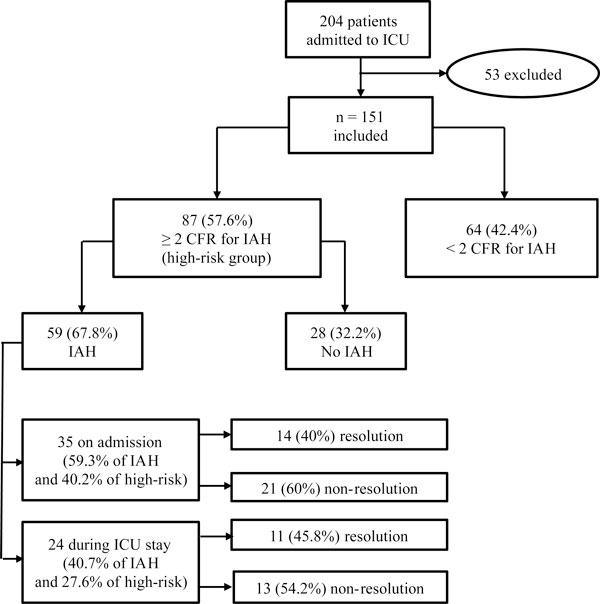
Prospective cohort study carried out at a medical ICU. A total of 151 medical patients were enrolled during a period of 3 months. After ICU whole staff training, we conducted daily screening of the four CRF for IAH based on the World Society of Abdominal Compartment Syndrome (WSACS) guidelines (namely, diminished abdominal wall compliance, increased intraluminal content, increased abdominal content, and capillary leak syndrome or fluid resuscitation). In those patients with risk factors of at least two different categories (≥2 CRF), intra-abdominal pressure (IAP) was measured every 8 h during ICU stay. Data included demographics, main diagnosis on admission, severity scores, cumulative fluid balance, daily mean IAP, resolution of IAH, days of ICU and hospital stay, and mortality.
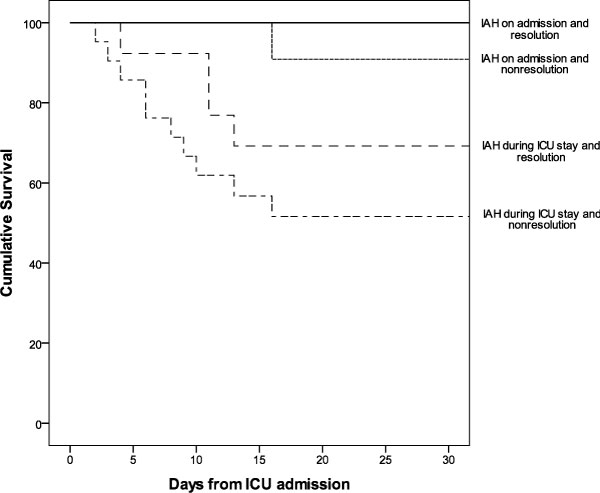
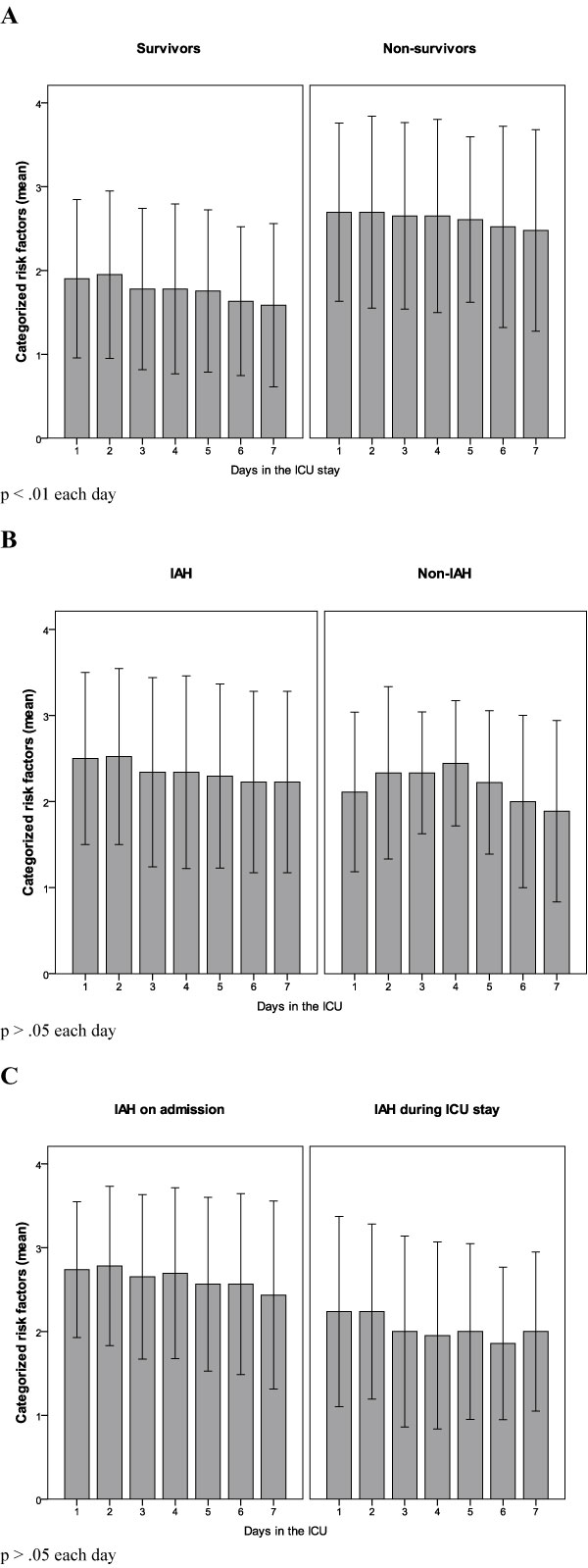
Eighty-seven patients (57.6%) had ≥2 CRF for IAH, 59 (67.8%) out of whom developed IAH. Patients with ≥2 CRF had a significantly higher mortality rate (41.4 vs. 14.3%, p < 0.001). Patients with IAH had higher body mass index, severity scores, organ dysfunctions/failures, number of CRF for IAH, days of ICU/hospital stay and hospital mortality rate (45.8 vs. 32.1%, p = 0.22). Non-resolution of IAH was associated with a higher mortality rate (64.7 vs. 35.3%, p = 0.001). None of the cohort patients developed abdominal compartment syndrome. The multivariate analysis showed that IAH development (odds ratio (OR) 4.09; 95% confidence interval (CI) 0.83-20.12) was a non-independent risk factor for mortality, and its non-resolution (OR 13.15; 95% CI 22.13-81.92) was an independent risk factor for mortality.
Critically ill medical patients admitted to ICU with ≥2 CRF have high morbidity, mortality rate, and incidence of IAH, so IAP should be measured and monitored as recommended by the WSACS. Our study highlights the importance of implementing screening and assessment protocols for an early diagnosis of IAH.
本研究旨在确定存在 2 种或以上腹腔高压(IAH)分类危险因素(CRF)的患者中 IAH 的发生率,以及这些患者在重症监护病房(ICU)期间的发病率和死亡率。
这是一项在医疗 ICU 进行的前瞻性队列研究。在 3 个月的时间内,共纳入了 151 名医疗患者。在 ICU 全体工作人员接受培训后,我们根据世界腹外科学会(WSACS)指南(即腹壁顺应性降低、腔内内容物增加、腹部内容物增加和毛细血管渗漏综合征或液体复苏),对这 4 种 IAH 的 CRF 进行了每日筛查。对于至少有 2 种不同类别的危险因素(≥2 CRF)的患者,在 ICU 住院期间每 8 小时测量一次腹腔内压(IAP)。数据包括人口统计学资料、入院时的主要诊断、严重程度评分、累计液体平衡、每日平均 IAP、IAH 缓解情况、ICU 和住院天数以及死亡率。
87 名(57.6%)患者存在≥2 种 IAH CRF,其中 59 名(67.8%)患者发生了 IAH。≥2 CRF 的患者死亡率显著更高(41.4%比 14.3%,p < 0.001)。发生 IAH 的患者体重指数、严重程度评分、器官功能障碍/衰竭、IAH 的 CRF 数量、ICU/住院天数和住院死亡率更高(45.8%比 32.1%,p = 0.22)。IAH 未缓解与更高的死亡率相关(64.7%比 35.3%,p = 0.001)。本队列患者中均未发生腹腔间隔室综合征。多变量分析显示,IAH 发生(比值比(OR)4.09;95%置信区间(CI)0.83-20.12)是非独立的死亡危险因素,IAH 未缓解(OR 13.15;95% CI 22.13-81.92)是独立的死亡危险因素。
入住 ICU 的存在≥2 种 CRF 的危重症医疗患者发病率、死亡率和 IAH 发生率均较高,因此应按照 WSACS 的建议测量和监测 IAP。我们的研究强调了实施筛查和评估方案以早期诊断 IAH 的重要性。