Department of Neonatology and Pediatric Intensive Care, Children's Hospital Dritter Orden, Bischof-Altmann-Str, 9, 94032 Passau, Germany.
Ann Intensive Care. 2012 Jul 5;2 Suppl 1(Suppl 1):S8. doi: 10.1186/2110-5820-2-S1-S8.
Several decades ago, the beneficial effects of goal-directed therapy, which include decompressive laparotomy (DL) and open abdomen procedures in cases of intra-abdominal hypertension (IAH) in children, were proven in the context of closures of abdominal wall defects and large-for-size organ transplantations. Different neonatologic and pediatric disease patterns are also known to be capable of increasing intra-abdominal pressure (IAP). Nevertheless, a considerable knowledge transfer regarding such risk factors has hardly taken place. When left undetected and untreated, IAH threatens to evolve into abdominal compartment syndrome (ACS), which is accompanied by a mortality rate of up to 60% in children. Therefore, the present study looks at the recognition and knowledge of IAH/ACS among German pediatric intensivists.
In June 2010, a questionnaire was mailed to the heads of pediatric intensive care units of 205 German pediatric hospitals.
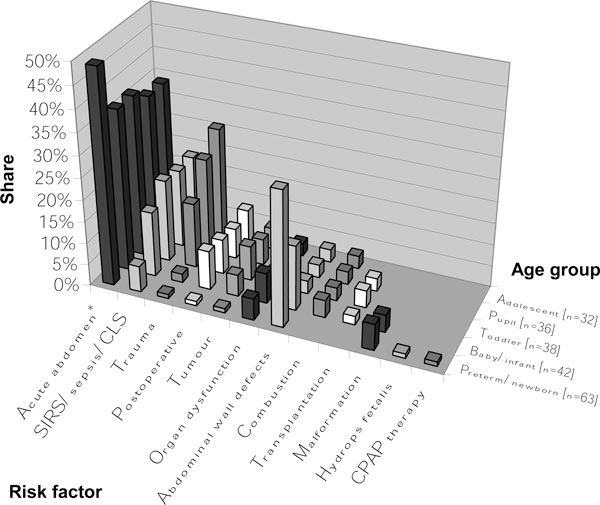
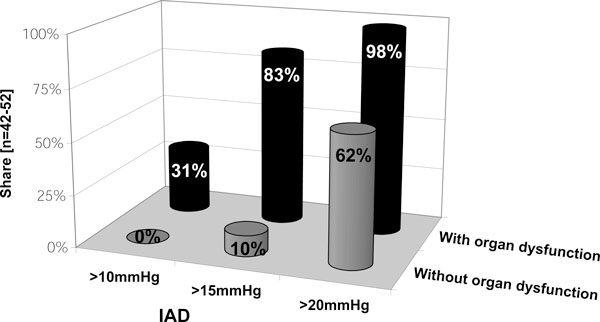
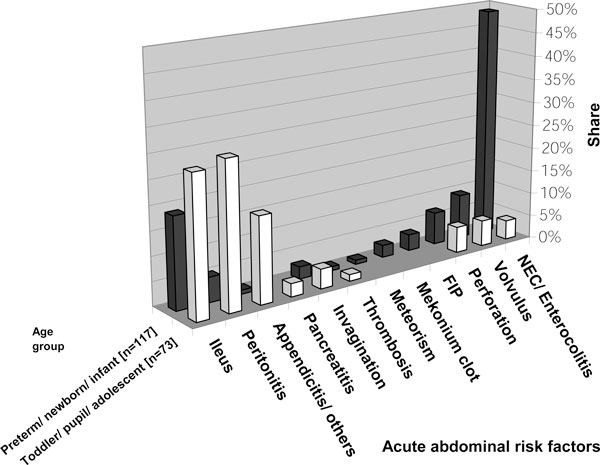
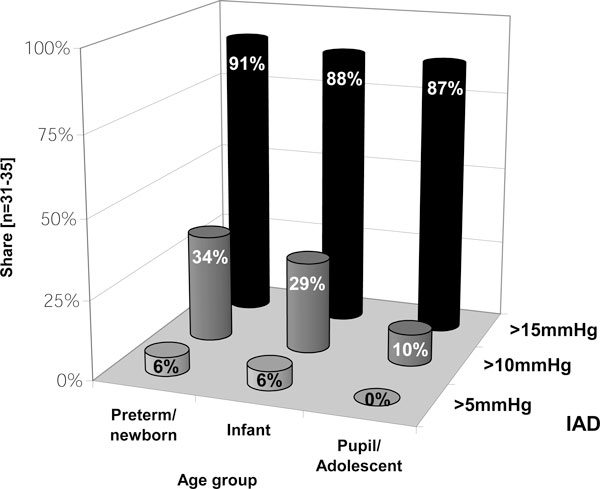
The response rate was 62%. At least one case of IAH was reported by 36% of respondents; at least one case of ACS, by 25%. Compared with adolescents, younger critically ill children appeared to develop IAH/ACS more often. Routine measurements of IAP were said to be performed by 20% of respondents. Bladder pressure was used most frequently (96%) to assess IAP. Some respondents (17%) only measured IAP in cases of organ dysfunction and failure. In 2009, the year preceding this study, 21% of respondents claimed to have performed a DL. Surgical decompression was indicated if signs of organ dysfunction were present. This was also done in cases of at least grade III IAH (IAP > 15 mmHg) without organ impairment.
Although awareness among pediatricians appears to have been increasing over the last decade, definitions and guidelines regarding the diagnosis and management of IAH/ACS are not applied uniformly. This variability could express an ever present lack of awareness and solid prospective data.
几十年前,目标导向治疗的有益效果在儿童腹腔内高压(IAH)的情况下得到了证明,包括减压剖腹术(DL)和开放性腹部手术,用于腹壁缺陷和大器官移植的关闭。不同的新生儿和儿科疾病模式也被认为能够增加腹腔内压力(IAP)。然而,关于这些危险因素的知识转移几乎没有发生。IAH 如果未被发现和治疗,可能会发展为腹间隔室综合征(ACS),儿童的死亡率高达 60%。因此,本研究着眼于德国儿科重症监护医师对 IAH/ACS 的认识和了解。
2010 年 6 月,向 205 家德国儿科医院的儿科重症监护病房主任邮寄了一份问卷。
回复率为 62%。36%的受访者报告至少有一例 IAH;25%的受访者报告至少有一例 ACS。与青少年相比,病情较重的儿童似乎更容易发生 IAH/ACS。20%的受访者表示会常规测量 IAP。膀胱压是最常使用的(96%)来评估 IAP。一些受访者(17%)仅在器官功能障碍和衰竭的情况下测量 IAP。在这项研究之前的 2009 年,21%的受访者声称进行了 DL。如果存在器官功能障碍的迹象,则进行手术减压。在没有器官损伤的情况下,即使存在至少 III 级 IAH(IAP>15mmHg)也会进行手术减压。
尽管儿科医生的意识在过去十年中似乎有所提高,但 IAH/ACS 的诊断和管理的定义和指南并未得到统一应用。这种可变性可能表达了始终存在的缺乏意识和可靠的前瞻性数据。