Junius-Walker Ulrike, Wrede Jennifer, Schleef Tanja, Diederichs-Egidi Heike, Wiese Birgitt, Hummers-Pradier Eva, Dierks Marie-Luise
Institute of General Practice, Hannover Medical School, Hannover, Germany.
BMC Res Notes. 2012 Aug 16;5:443. doi: 10.1186/1756-0500-5-443.
GPs increasingly deal with multiple health problems of their older patients. They have to apply a hierarchical management approach that considers priorities to balance competing needs for treatment. Yet, the practice of setting individual priorities in older patients is largely unexplored. This paper analyses the GPs' perceptions on important and unimportant health problems and how these affect their treatment.
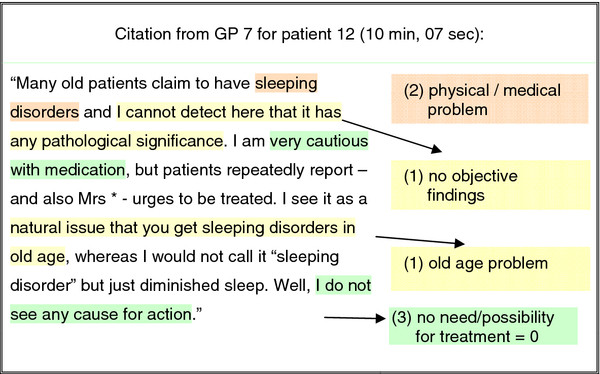
GPs appraised the importance of health problems for a purposive sample of their older patients in semi-structured interviews. Prior to the interviews, the GPs had received a list of their patients' health problems resulting from a geriatric assessment and were asked to rate the importance of each identified problem. In the interviews the GPs subsequently explained why they considered certain health problems important or not and how this affected treatment. Data was analysed using qualitative content analysis and quantitative methods.
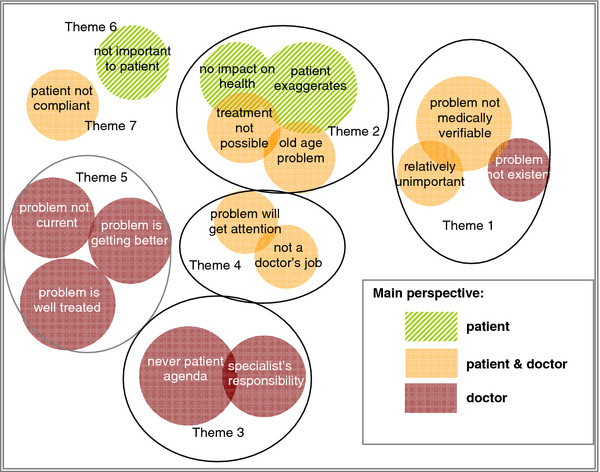
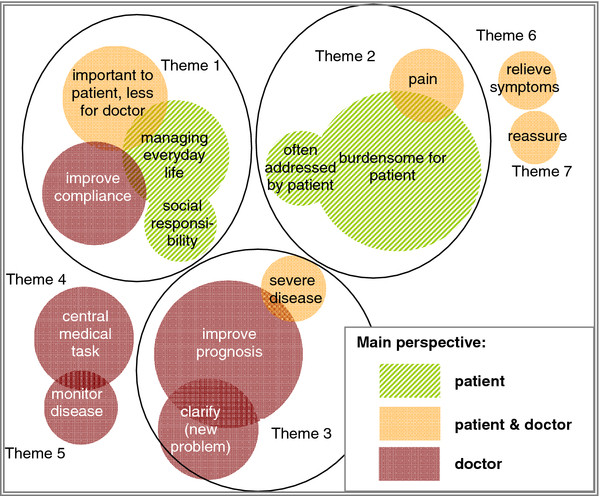
The problems GPs perceive as important are those that are medical and require active treatment or monitoring, or that induce empathy or awareness but cannot be assisted further. Unimportant problems are those that are well managed problems and need no further attention as well as age-related conditions or functional disabilities that provoke fatalism, or those considered outside the GPs' responsibility. Statements of professional actions are closely linked to explanations of important problems and relate to physical problems rather than functional and social patient issues.
GPs tend to prioritise treatable clinical conditions. Treatment approaches are, however, vague or missing for complex chronic illnesses and disabilities. Here, patient empowerment strategies are of value and need to be developed and implemented. The professional concepts of ageing and disability should not impede but rather foster treatment and care. To this end, GPs need to be able to delegate care to a functioning primary care team.
German Trial Register (DRKS): 00000792.
全科医生越来越多地应对老年患者的多种健康问题。他们必须采用一种分层管理方法,考虑优先事项以平衡相互竞争的治疗需求。然而,在老年患者中确定个人优先事项的做法在很大程度上尚未得到探索。本文分析了全科医生对重要和不重要健康问题的看法以及这些看法如何影响他们的治疗。
全科医生在半结构化访谈中对其老年患者的一个有目的样本的健康问题的重要性进行评估。在访谈之前,全科医生收到了一份由老年评估得出的患者健康问题清单,并被要求对每个已确定问题的重要性进行评分。在访谈中,全科医生随后解释了他们为什么认为某些健康问题重要或不重要以及这如何影响治疗。使用定性内容分析和定量方法对数据进行分析。
全科医生认为重要的问题是那些属于医疗范畴且需要积极治疗或监测的问题,或者是那些引发同理心或意识但无法进一步提供帮助的问题。不重要的问题是那些管理良好且无需进一步关注的问题,以及引发宿命论的与年龄相关的状况或功能障碍,或者是那些被认为超出全科医生职责范围的问题。专业行动的陈述与对重要问题的解释密切相关,并且与身体问题而非患者的功能和社会问题相关。
全科医生倾向于优先处理可治疗的临床病症。然而,对于复杂的慢性疾病和残疾,治疗方法模糊或缺失。在此,患者赋权策略具有价值,需要加以制定和实施。衰老和残疾的专业概念不应阻碍而应促进治疗和护理。为此,全科医生需要能够将护理工作委托给一个运作良好的初级保健团队。
德国试验注册库(DRKS):00000792。