Pfizer Oncology, La Jolla, CA, USA.
J Transl Med. 2012 Aug 16;10:165. doi: 10.1186/1479-5876-10-165.
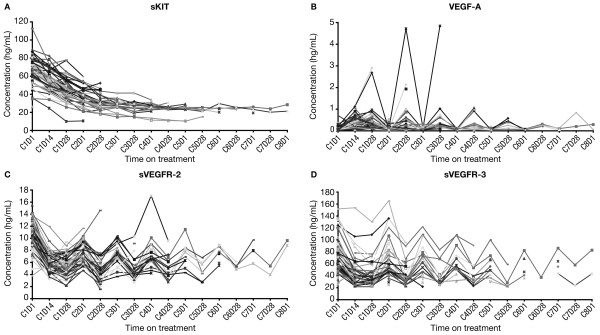
Sunitinib inhibits vascular endothelial growth factor receptors (VEGFRs), platelet-derived growth factor receptors, and stem cell factor receptor (KIT). The ability of soluble (s)KIT, VEGF-A, sVEGFR-2, and sVEGFR-3 to predict clinical outcome was analyzed in 61 patients with previously treated metastatic breast cancer (MBC) in a phase II study of sunitinib monotherapy (ClinicalTrials.gov NCT00078000).
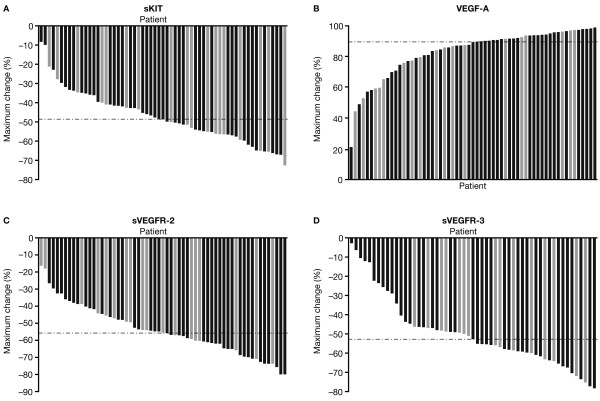
Plasma concentrations of soluble proteins were measured at baseline and during treatment with sunitinib 50 mg/day (4 weeks on treatment, 2 weeks off treatment). Baseline concentrations and maximal percent change during the first two treatment cycles were stratified by median values and evaluated for correlation with median time to tumor progression (TTP) and overall survival (OS). This latter fixed time period was chosen to avoid bias accruing from patients who were on study for longer periods of time.
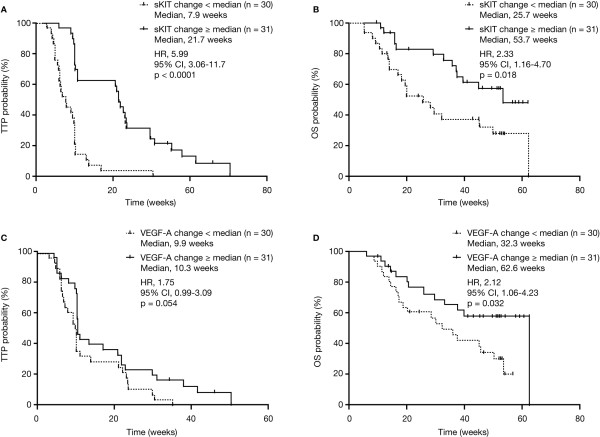
TTP was significantly longer in patients having median or higher maximal percent sKIT change compared with patients with less than the median change (21.7 vs. 7.9 weeks; p < 0.0001). Similarly, OS was significantly longer in patients having median or higher sKIT change versus less than the median change (53.7 vs. 25.7 weeks; p = 0.018). Significant prolongation of OS (62.6 vs. 32.3 weeks; p = 0.032), but not TTP, was observed in patients with a median or higher maximal percent VEGF-A change compared with less than the median change. Maximal percent change of sVEGFR-2 or sVEGFR-3 concentrations and baseline concentrations of all four proteins were not predictive of clinical outcome.
This exploratory analysis suggests that changes in sKIT and possibly VEGF-A early during sunitinib treatment may be predictive of clinical outcome in MBC.
舒尼替尼抑制血管内皮生长因子受体(VEGFRs)、血小板衍生生长因子受体和干细胞因子受体(KIT)。在一项舒尼替尼单药治疗 61 例转移性乳腺癌(MBC)患者的 II 期研究中,分析了可溶性(s)KIT、VEGF-A、sVEGFR-2 和 sVEGFR-3 预测临床结局的能力(ClinicalTrials.gov NCT00078000)。
在舒尼替尼 50mg/天治疗期间(治疗 4 周,停药 2 周),分别于基线和治疗期间测量血浆可溶性蛋白浓度。根据中位数值对基线浓度和前两个治疗周期中的最大百分比变化进行分层,并评估其与中位肿瘤进展时间(TTP)和总生存(OS)的相关性。选择这个固定的时间段是为了避免由于患者在研究中观察时间较长而导致的偏倚。
与 sKIT 变化小于中位数的患者相比,sKIT 最大百分比变化中位数或更高的患者 TTP 明显更长(21.7 与 7.9 周;p<0.0001)。同样,sKIT 变化中位数或更高的患者 OS 明显长于 sKIT 变化小于中位数的患者(53.7 与 25.7 周;p=0.018)。与 sKIT 变化小于中位数的患者相比,sKIT 最大百分比变化中位数或更高的患者 OS 显著延长(62.6 与 32.3 周;p=0.032),但 TTP 无显著延长。sVEGFR-2 或 sVEGFR-3 浓度的最大百分比变化和所有四种蛋白的基线浓度均不能预测临床结局。
这项探索性分析表明,在舒尼替尼治疗早期 sKIT 和可能 VEGF-A 的变化可能是 MBC 临床结局的预测因素。