Department of Intensive Care Medicine, Chi Mei Medical Center, Yong-Kang City, Tainan, Taiwan.
BMC Gastroenterol. 2012 Aug 17;12:112. doi: 10.1186/1471-230X-12-112.
We investigated the relation between hospital volume and outcome in patients with severe acute pancreatitis (SAP). The determination is important because patient outcome may be improved through volume-based selective referral.
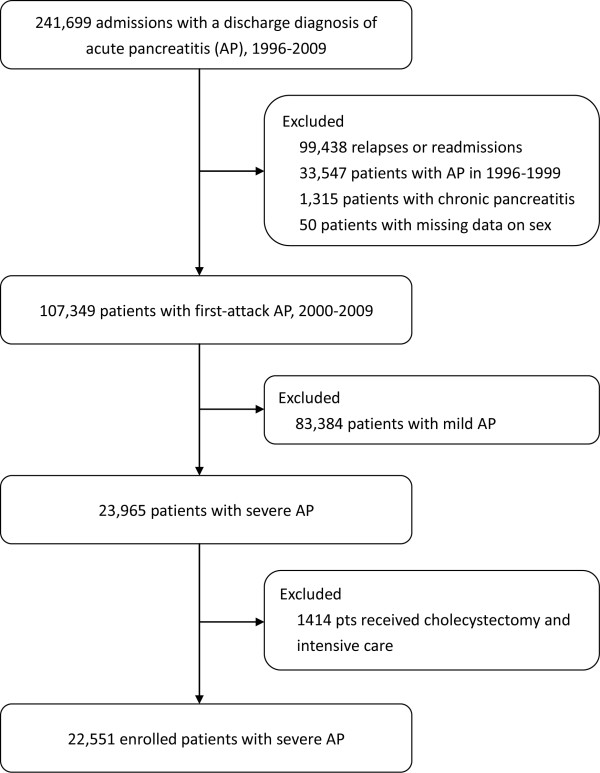
In this cohort study, we analyzed 22,551 SAP patients in 2,208 hospital-years (between 2000 and 2009) from Taiwan's National Health Insurance Research Database. Primary outcome was hospital mortality. Secondary outcomes were hospital length of stay and charges. Hospital SAP volume was measured both as categorical and as continuous variables (per one case increase each hospital-year). The effect was assessed using multivariable logistic regression models with generalized estimating equations accounting for hospital clustering effect. Adjusted covariates included patient and hospital characteristics (model 1), and additional treatment variables (model 2).
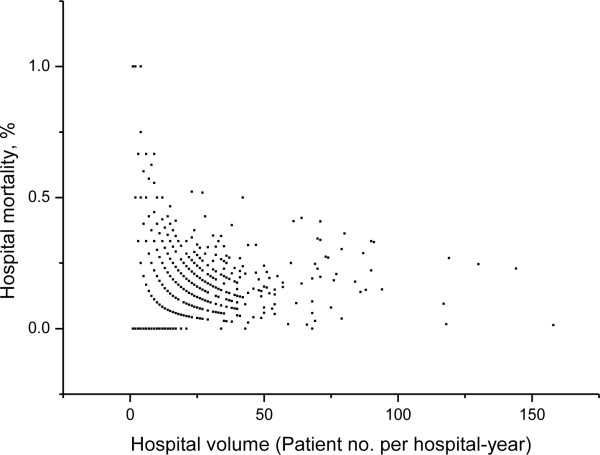
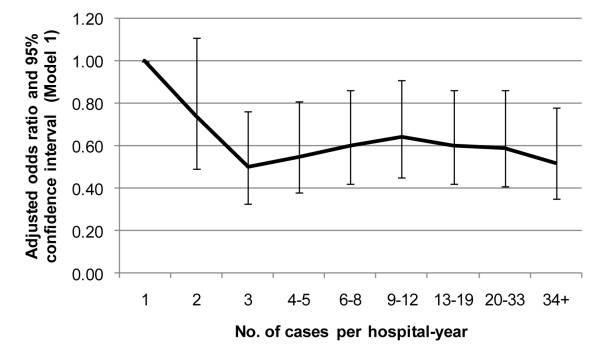
Irrespective of the measurements, increasing hospital volume was associated with reduced risk of hospital mortality after adjusting the patient and hospital characteristics (adjusted odds ratio [OR] 0.995, 95% confidence interval [CI] 0.993-0.998 for per one case increase). The patients treated in the highest volume quartile (≥14 cases per hospital-year) had 42% lower risk of hospital mortality than those in the lowest volume quartile (1 case per hospital-year) after adjusting the patient and hospital characteristics (adjusted OR 0.58, 95% CI 0.40-0.83). However, an inverse relation between volume and hospital stay or hospital charges was observed only when the volume was analyzed as a categorical variable. After adjusting the treatment covariates, the volume effect on hospital mortality disappeared regardless of the volume measures.
These findings support the use of volume-based selective referral for patients with SAP and suggest that differences in levels or processes of care among hospitals may have contributed to the volume effect.
我们研究了严重急性胰腺炎(SAP)患者的医院容量与结局之间的关系。这种确定很重要,因为通过基于容量的选择性转诊,患者的结局可能会得到改善。
在这项队列研究中,我们分析了来自台湾全民健康保险研究数据库的 22551 例 SAP 患者的 2208 个医院年(2000 年至 2009 年)。主要结局是医院死亡率。次要结局是医院住院时间和费用。医院 SAP 容量既作为分类变量又作为连续变量(每个医院年增加一个病例)进行测量。使用具有广义估计方程的多变量逻辑回归模型来评估效果,该模型考虑了医院聚类效应。调整的协变量包括患者和医院特征(模型 1)以及额外的治疗变量(模型 2)。
无论采用何种测量方法,在调整患者和医院特征后,随着医院容量的增加,医院死亡率的风险降低(每增加一个病例,调整后的优势比 [OR] 为 0.995,95%置信区间 [CI] 为 0.993-0.998)。在调整患者和医院特征后,与容量最低的四分位数(每个医院年 1 例)相比,容量最高的四分位数(≥14 例/医院年)的患者的医院死亡率降低了 42%(调整后的 OR 为 0.58,95% CI 为 0.40-0.83)。然而,仅当容量作为分类变量进行分析时,才观察到容量与住院时间或住院费用之间的反比关系。在调整治疗协变量后,无论使用何种容量测量方法,容量对医院死亡率的影响均消失。
这些发现支持使用基于容量的选择性转诊来治疗 SAP 患者,并表明医院之间的护理水平或护理过程的差异可能导致了容量效应。