Department of Radiation Oncology, Dana Farber Cancer Institute, and Brigham and Women's Hospital, Harvard Medical School, Boston, Massachusetts 02115, USA.
J Urol. 2012 Oct;188(4):1151-6. doi: 10.1016/j.juro.2012.06.010. Epub 2012 Aug 15.
We report updated results of magnetic resonance imaging guided partial prostate brachytherapy and propose a definition of biochemical failure following focal therapy.
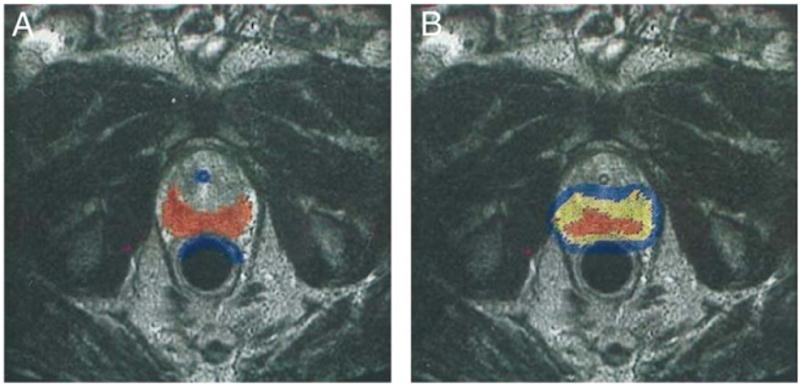
From 1997 to 2007, 318 men with cT1c, prostate specific antigen less than 15 ng/ml, Gleason 3 + 4 or less prostate cancer received magnetic resonance imaging guided brachytherapy in which only the peripheral zone was targeted. To exclude benign prostate specific antigen increases due to prostatic hyperplasia, we investigated the usefulness of defining prostate specific antigen failure as nadir +2 with prostate specific antigen velocity greater than 0.75 ng/ml per year. Cox regression was used to determine the factors associated with prostate specific antigen failure.
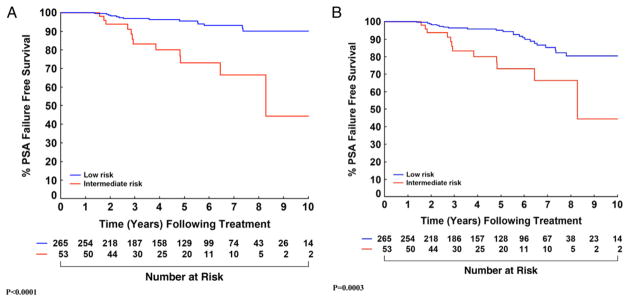
Median followup was 5.1 years (maximum 12.1). While 36 patients met the nadir +2 criteria, 16 of 17 biopsy proven local recurrences were among the 26 men who also had a prostate specific antigen velocity greater than 0.75 ng/ml per year (16 of 26 vs 1 of 10, p = 0.008). Using the nadir +2 definition, prostate specific antigen failure-free survival for low risk cases at 5 and 8 years was 95.1% (91.0-97.3) and 80.4% (70.7-87.1), respectively. This rate improved to 95.6% (91.6-97.7) and 90.0% (82.6-94.3) using nadir +2 with prostate specific antigen velocity greater than 0.75 ng/ml per year. For intermediate risk cases survival was 73.0% (55.0-84.8) at 5 years and 66.4% (44.8-81.1) at 8 years (the same values as using nadir +2 with prostate specific antigen velocity greater than 0.75 ng/ml per year).
Requiring a prostate specific antigen velocity greater than 0.75 ng/ml per year in addition to nadir +2 appears to better predict clinical failure after therapies that target less than the whole gland. Further followup will determine whether magnetic resonance imaging guided brachytherapy targeting the peripheral zone produces comparable cancer control to whole gland treatment in men with low risk disease. However, at this time it does not appear adequate for men with even favorable intermediate risk disease.
我们报告了磁共振成像引导下前列腺部分切除术的最新结果,并提出了局灶性治疗后生化失败的定义。
1997 年至 2007 年,318 例 cT1c、前列腺特异性抗原(PSA)<15ng/ml、Gleason 评分 3+4 或更低的前列腺癌患者接受了磁共振成像引导下的前列腺部分切除术,仅靶向外周区。为了排除由于前列腺增生引起的良性 PSA 升高,我们研究了将 PSA 失败定义为 PSA 速度大于 0.75ng/ml/年时的 PSA 下降 2 个标准差的有效性。Cox 回归用于确定与 PSA 失败相关的因素。
中位随访时间为 5.1 年(最长 12.1 年)。虽然有 36 例患者符合 PSA 下降 2 个标准差的标准,但在 17 例经活检证实的局部复发患者中,有 16 例患者的 PSA 速度大于 0.75ng/ml/年(26 例中有 16 例,10 例中有 1 例,p=0.008)。使用 PSA 下降 2 个标准差的定义,低危病例的 5 年和 8 年 PSA 无失败生存率分别为 95.1%(91.0-97.3)和 80.4%(70.7-87.1)。如果 PSA 速度大于 0.75ng/ml/年,则该生存率提高至 95.6%(91.6-97.7)和 90.0%(82.6-94.3)。对于中危病例,5 年时的生存率为 73.0%(55.0-84.8),8 年时为 66.4%(44.8-81.1)(与 PSA 速度大于 0.75ng/ml/年时使用 PSA 下降 2 个标准差的结果相同)。
在 PSA 下降 2 个标准差的基础上,还需要 PSA 速度大于 0.75ng/ml/年,这似乎可以更好地预测靶向整个腺体以下治疗后的临床失败。进一步的随访将确定磁共振成像引导下仅靶向外周区的前列腺部分切除术是否能在低危疾病患者中产生与全腺体治疗相当的癌症控制效果。然而,目前对于即使是中危的患者来说,这似乎还不够。