Bragadottir Gudrun, Redfors Bengt, Ricksten Sven-Erik
Crit Care. 2012 Aug 17;16(4):R159. doi: 10.1186/cc11480.
Acute kidney injury (AKI), which is a major complication after cardiovascular surgery, is associated with significant morbidity and mortality. Diuretic agents are frequently used to improve urine output and to facilitate fluid management in these patients. Mannitol, an osmotic diuretic, is used in the perioperative setting in the belief that it exerts reno-protective properties. In a recent study on uncomplicated postcardiac-surgery patients with normal renal function, mannitol increased glomerular filtration rate (GFR), possibly by a deswelling effect on tubular cells. Furthermore, experimental studies have previously shown that renal ischemia causes an endothelial cell injury and dysfunction followed by endothelial cell edema. We studied the effects of mannitol on renal blood flow (RBF), glomerular filtration rate (GFR), renal oxygen consumption (RVO2), and extraction (RO2Ex) in early, ischemic AKI after cardiac surgery.
Eleven patients with AKI were studied during propofol sedation and mechanical ventilation 2 to 6 days after complicated cardiac surgery. All patients had severe heart failure treated with one (100%) or two (73%) inotropic agents and intraaortic balloon pump (36%). Systemic hemodynamics were measured with a pulmonary artery catheter. RBF and renal filtration fraction (FF) were measured by the renal vein thermo-dilution technique and by renal extraction of chromium-51-ethylenediaminetetraacetic acid (51Cr-EDTA), respectively. GFR was calculated as the product of FF and renal plasma flow RBF × (1-hematocrit). RVO2 and RO2Ex were calculated from arterial and renal vein blood samples according to standard formulae. After control measurements, a bolus dose of mannitol, 225 mg/kg, was given, followed by an infusion at a rate of 75 mg/kg/h for two 30-minute periods.
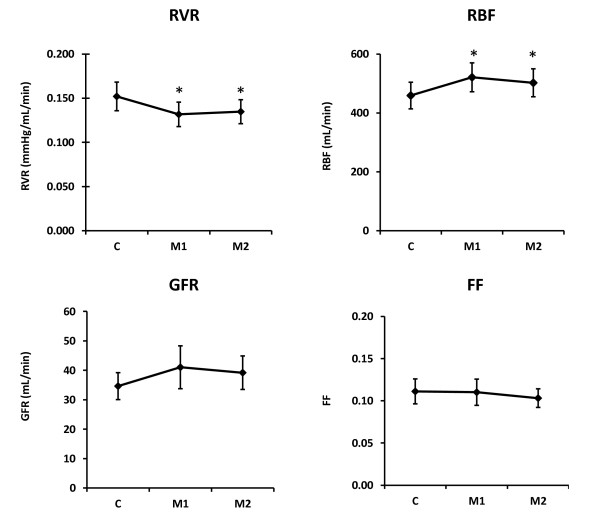
Mannitol did not affect cardiac index or cardiac filling pressures. Mannitol increased urine flow by 61% (P < 0.001). This was accompanied by a 12% increase in RBF (P < 0.05) and a 13% decrease in renal vascular resistance (P < 0.05). Mannitol increased the RBF/cardiac output (CO) relation (P = 0.040). Mannitol caused no significant changes in RO2Ext or renal FF.
Mannitol treatment of postoperative AKI induces a renal vasodilation and redistributes systemic blood flow to the kidneys. Mannitol does not affect filtration fraction or renal oxygenation, suggestive of balanced increases in perfusion/filtration and oxygen demand/supply.
急性肾损伤(AKI)是心血管手术后的一种主要并发症,与显著的发病率和死亡率相关。利尿剂常用于改善这些患者的尿量并促进液体管理。甘露醇作为一种渗透性利尿剂,在围手术期使用,人们认为它具有肾脏保护作用。在最近一项针对心脏手术后肾功能正常的非复杂性患者的研究中,甘露醇增加了肾小球滤过率(GFR),可能是通过对肾小管细胞的消肿作用。此外,先前的实验研究表明,肾脏缺血会导致内皮细胞损伤和功能障碍,随后出现内皮细胞水肿。我们研究了甘露醇对心脏手术后早期缺血性AKI患者肾血流量(RBF)、肾小球滤过率(GFR)、肾脏氧耗(RVO2)和摄取(RO2Ex)的影响。
对11例AKI患者在复杂心脏手术后2至6天接受丙泊酚镇静和机械通气期间进行研究。所有患者均患有严重心力衰竭,使用一种(100%)或两种(73%)血管活性药物及主动脉内球囊泵治疗(36%)。使用肺动脉导管测量全身血流动力学。RBF和肾滤过分数(FF)分别通过肾静脉热稀释技术和51铬 - 乙二胺四乙酸(51Cr - EDTA)肾摄取法测量。GFR计算为FF与肾血浆流量RBF×(1 - 血细胞比容)的乘积。RVO2和RO2Ex根据标准公式从动脉和肾静脉血样中计算得出。在进行对照测量后,给予225 mg/kg的甘露醇推注剂量,随后以75 mg/kg/h的速率输注两个30分钟时间段。
甘露醇不影响心脏指数或心脏充盈压。甘露醇使尿量增加61%(P < 0.001)。这伴随着RBF增加12%(P < 0.05)和肾血管阻力降低13%(P < 0.05)。甘露醇增加了RBF/心输出量(CO)关系(P = 0.040)。甘露醇对RO2Ext或肾FF无显著影响。
甘露醇治疗术后AKI可诱导肾血管舒张并将全身血流重新分配至肾脏。甘露醇不影响滤过分数或肾脏氧合,提示灌注/滤过和氧需求/供应平衡增加。