Unidade de tuberculose, Servizo de Medicina Interna, Complexo hospitalario de Pontevedra, SERGAS, Mourente s/n, Pontevedra 36071, Spain.
BMC Infect Dis. 2012 Aug 20;12:195. doi: 10.1186/1471-2334-12-195.
Patients with end-stage renal disease (ESRD) and Mycobacterium tuberculosis infection pose a high risk of developing active TB disease. It is therefore important to detect latent TB infection (LTBI) to be able to offer treatment and prevent progression to TB disease. We assessed the value of the tuberculin skin test (TST) and of an interferon-gamma release assay (Quantiferon®-TB Gold in-Tube, QFT) for diagnosing LTBI in ESRD patients, after prolonged exposure to a highly contagious TB case in a haemodialysis unit. As a high number of patients presented erythema without induration in the TST response, this type of reaction was also analysed.
The TST and QFT were simultaneously performed twelve weeks after the last possible exposure to a bacilliferous TB patient. If the first TST (TST-1) was negative, a second TST (TST-2) was performed 15 days later to detect a booster response. A comparison was made between the TST responses (including those cases with erythema without induration) and those for the QFT. The correlation with risk of infection and the concordance between tests were both analysed.
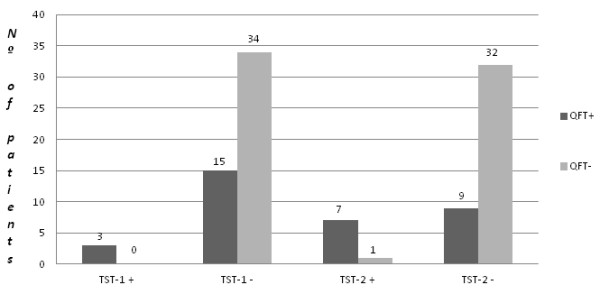
A total of 52 patients fulfilled the inclusion criteria. Overall, 11 patients (21.2%) had a positive TST response: 3 for TST-1 and 8 for TST-2, and 18 patients (34.6%) showed a positive QFT response (p = 0.065). Erythema without induration was found in 3 patients at TST-1 and in a further 9 patients at TST-2. The three patients with erythema without induration in TST-1 had a positive TST-2 response. Concordance between TST and QFT was weak for TST-1 (κ = 0.21); it was moderate for overall TST (κ = 0.49); and it was strong if both induration and erythema (κ = 0.67) were considered.
In patients with ESRD, erythema without induration in the TST response could potentially be an indicator of M. tuberculosis infection. The QFT shows better accuracy for LTBI diagnosis than the TST.
患有终末期肾病(ESRD)和结核分枝杆菌感染的患者有很高的发展为活动性结核病的风险。因此,检测潜伏性结核感染(LTBI)并提供治疗以防止进展为结核病是很重要的。我们评估了结核菌素皮肤试验(TST)和干扰素-γ释放试验(QuantiFERON®-TB Gold In-Tube,QFT)在血液透析单位中接触高度传染性结核病例后对诊断 ESRD 患者 LTBI 的价值。由于 TST 反应中有大量患者出现红斑而无硬结,因此也分析了这种类型的反应。
在最后一次接触有传染性的结核患者后 12 周,同时进行 TST 和 QFT。如果第一次 TST(TST-1)为阴性,则在 15 天后进行第二次 TST(TST-2)以检测增强反应。将 TST 反应(包括红斑而无硬结的病例)与 QFT 进行比较。分析了与感染风险的相关性以及测试之间的一致性。
共有 52 名患者符合纳入标准。总的来说,有 11 名患者(21.2%)TST 反应阳性:3 名 TST-1,8 名 TST-2,18 名患者(34.6%)QFT 反应阳性(p=0.065)。TST-1 时发现 3 例有红斑而无硬结,TST-2 时发现另外 9 例有红斑而无硬结。TST-1 时红斑而无硬结的 3 名患者 TST-2 反应阳性。TST-1 时 TST 和 QFT 之间的一致性较弱(κ=0.21);总体 TST 时中度一致(κ=0.49);如果同时考虑硬结和红斑,则一致性较强(κ=0.67)。
在 ESRD 患者中,TST 反应中的红斑而无硬结可能是结核分枝杆菌感染的潜在指标。QFT 比 TST 更准确地诊断 LTBI。