VU University medical center, EMGO Institute for Health and Care Research, Department of Public and Occupational Health, Amsterdam, the Netherlands.
BMC Fam Pract. 2012 Aug 22;13:89. doi: 10.1186/1471-2296-13-89.
Many patients are transferred from home to hospital during the final phase of life and the majority die in hospital. The aim of the study is to explore hospital referrals of palliative care patients for whom an out-of-hours general practitioner was called.
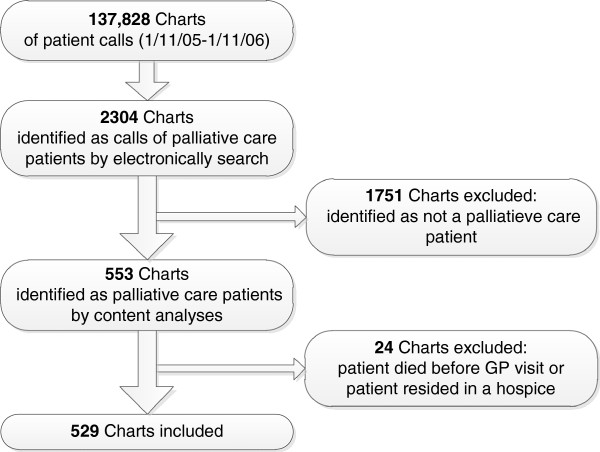
A retrospective descriptive chart study was conducted covering a one-year period (1/Nov/2005 to 1/Nov/2006) in all eight out-of-hours GP co-operatives in the Amsterdam region (Netherlands). All symptoms, sociodemographic and medical characteristics were recorded in 529 charts for palliative care patients. Multivariate logistic regression analysis was performed to identify the variables associated with hospital referrals at the end of life.
In all, 13% of all palliative care patients for whom an out-of-hours general practitioner was called were referred to hospital. Palliative care patients with cancer (OR 5,1), cardiovascular problems (OR 8,3), digestive problems (OR 2,5) and endocrine, metabolic and nutritional (EMN) problems (OR 2,5) had a significantly higher chance of being referred. Patients receiving professional nursing care (OR 0,2) and patients for whom their own general practitioner had transferred information to the out-of-hours cooperative (OR 0,4) had a significantly lower chance of hospital referral. The most frequent reasons for hospital referral, as noted by the out-of-hours general practitioner, were digestive (30%), EMN (19%) and respiratory (17%) problems.
Whilst acknowledging that an out-of-hours hospital referral can be the most desirable option in some situations, this study provides suggestions for avoiding undesirable hospital referrals by out-of-hours general practitioners at the end of life. These include anticipating digestive, EMN, respiratory and cardiovascular symptoms in palliative care patients.
许多患者在生命末期从家中转至医院,其中大多数患者在医院去世。本研究旨在探讨为已呼叫夜间全科医生的姑息治疗患者安排医院转诊的情况。
本研究为回顾性描述性图表研究,涵盖阿姆斯特丹地区(荷兰)8 家夜间全科医生合作机构的一年时间(2005 年 11 月 1 日至 2006 年 11 月 1 日)。所有姑息治疗患者的症状、社会人口学和医学特征均记录在 529 份图表中。采用多变量逻辑回归分析来确定与临终时医院转诊相关的变量。
总共,呼叫夜间全科医生的所有姑息治疗患者中,有 13%被转诊至医院。患有癌症(OR5.1)、心血管问题(OR8.3)、消化问题(OR2.5)和内分泌、代谢和营养(EMN)问题(OR2.5)的姑息治疗患者被转诊的可能性显著更高。接受专业护理(OR0.2)和其自身全科医生已将信息转至夜间合作机构的患者(OR0.4)被转诊至医院的可能性显著更低。夜间全科医生记录的转诊最常见原因是消化(30%)、EMN(19%)和呼吸(17%)问题。
尽管夜间医院转诊在某些情况下可能是最理想的选择,但本研究为夜间全科医生在临终时避免不必要的医院转诊提供了建议。这些建议包括预测姑息治疗患者的消化、EMN、呼吸和心血管症状。