Mingfeng He, Zhixin Wu, Qihong Guo, Lianda Li, Yanbin Yang, Jinfang Feng
Ann Indian Acad Neurol. 2012 Jul;15(3):191-5. doi: 10.4103/0972-2327.99713.
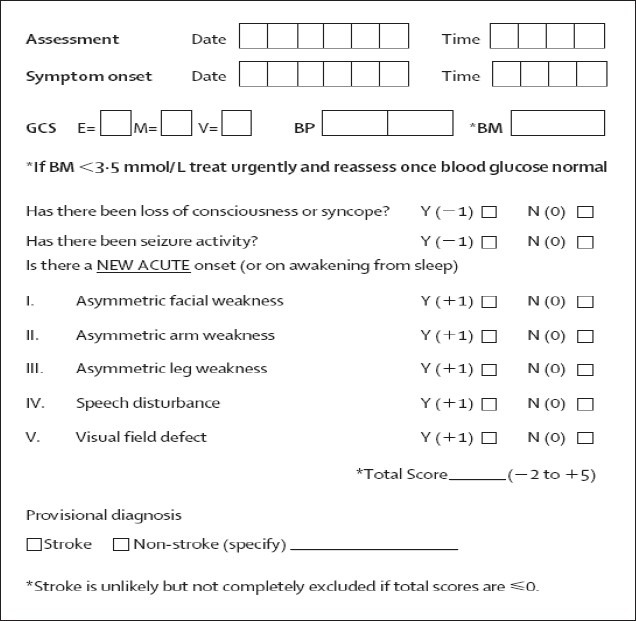
To determine the utility of the Recognition of Stroke in the Emergency Room (ROSIER) scale as a stroke recognition tool among Chinese patients in the prehospital setting.
Compared with the Cincinnati Prehospital Stroke Scale (CPSS), emergency physicians prospectively used the ROSIER as a stroke recognition tool on suspected patients in the prehospital setting. And, the final discharge diagnosis of stroke or transient ischemic attack made by neurologists, after assessment and review of clinical symptomatology and brain imaging findings, was used as the reference standard for diagnosis in the study. Then, the ROSIER and the CPSS like sensitivity (Se), specificity (Sp), positive predictive value (PPV), negative predictive value (NPV), related coefficient (r) and Kappa value were calculated.
In this study, 540 of 582 suspected stroke patients met the study criteria. The CPSS showed a diagnostic Se of 88.77% (95% confidence intervals [CI] 86.11-91.43%), Sp of 68.79% (95% CI 64.88-72.70%), PPV of 87.40% (95% CI 85.97-88.83%), NPV of 71.52% (95% CI 67.71-75.33%) and r of 0.503. Relatively, the ROSIER showed a diagnostic Se of 89.97% (95% CI 87.44-92.64%), Sp of 83.23% (95% CI 80.08-86.38%), PPV of 92.66% (95% CI 90.46-94.86%), NPV of 77.91% (95% CI 74.41-81.41%) and r of 0.584. According to the final discharge diagnosis, both the ROSIER and the CPSS were associated with the final discharge diagnosis (P < 0.05).The Kappa statistic value of the ROSIER and the CPSS were 0.718 and 0.582, respectively. However, there was no statistical significance of the positive rate between the ROSIER and the CPSS in this study (P > 0.05).
The ROSIER is a sensitive and specific stroke recognition tool for health providers' use among Chinese patients in the prehospital setting. However, it cannot be used to confidently rule out or identify stroke as a diagnosis. Comprehensive clinical assessment and further examination on potential stroke patients are still important and cannot be replaced. When it is difficult to objectively complete the ROSIER for patients, the CPSS could replace it in the prehospital setting.
确定急诊室卒中识别(ROSIER)量表作为院前环境中中国患者卒中识别工具的效用。
与辛辛那提院前卒中量表(CPSS)相比,急诊医生在前院环境中对疑似患者前瞻性地使用ROSIER作为卒中识别工具。并且,由神经科医生在评估和审查临床症状及脑影像学检查结果后做出的卒中或短暂性脑缺血发作的最终出院诊断,被用作该研究中的诊断参考标准。然后,计算ROSIER和CPSS的灵敏度(Se)、特异度(Sp)、阳性预测值(PPV)、阴性预测值(NPV)、相关系数(r)和Kappa值。
在本研究中,582例疑似卒中患者中有540例符合研究标准。CPSS显示诊断灵敏度为88.77%(95%置信区间[CI]86.11 - 91.43%),特异度为68.79%(95%CI 64.88 - 72.70%),阳性预测值为87.40%(95%CI 85.97 - 88.83%),阴性预测值为71.52%(95%CI 67.71 - 75.33%),r为0.503。相对而言,ROSIER显示诊断灵敏度为89.97%(95%CI 87.44 - 92.64%),特异度为83.23%(95%CI 80.08 - 86.38%),阳性预测值为92.66%(95%CI 90.46 - 94.86%),阴性预测值为77.91%(95%CI 74.41 - 81.41%),r为0.584。根据最终出院诊断,ROSIER和CPSS均与最终出院诊断相关(P < 0.05)。ROSIER和CPSS的Kappa统计值分别为0.718和0.582。然而,本研究中ROSIER和CPSS之间的阳性率无统计学意义(P > 0.05)。
ROSIER是一种敏感且特异的卒中识别工具,可供医护人员用于院前环境中的中国患者。然而,它不能用于可靠地排除或确诊卒中。对潜在卒中患者进行全面的临床评估和进一步检查仍然很重要且不可替代。当难以客观地为患者完成ROSIER时,CPSS可在前院环境中替代它。