Department of Medicine, Calgary, Alberta, Canada.
BMC Health Serv Res. 2012 Aug 30;12:290. doi: 10.1186/1472-6963-12-290.
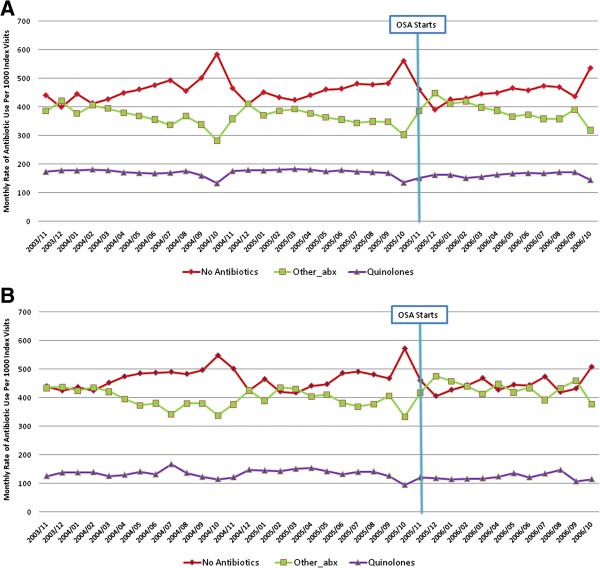
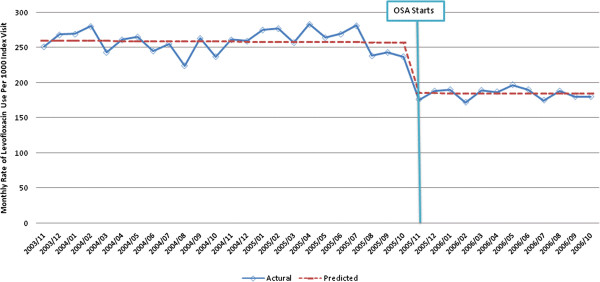
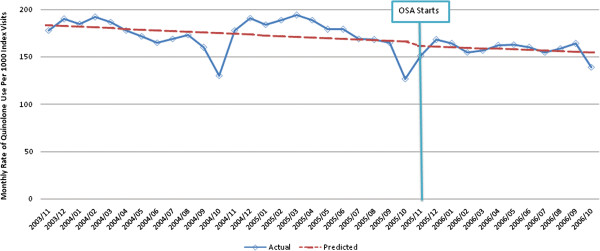
Publicly-funded drug plans often use prior authorization policies to limit drug prescribing. To guide physician prescribing of a class of antibiotics with broad antimicrobial activity (quinolone antibiotics) in accordance with new prescribing guidelines, Alberta's provincial health ministry implemented a new mechanism for formulary restriction entitled the optional special authorization (OSA) program. We conducted an observational study to determine the impact of this new formulary restriction policy on antimicrobial prescription rates as well as any clinical consequences.
Quinolone antibiotic use, and adherence with quinolone prescribing guidelines, was assessed before and after implementation of the OSA program in patients with common outpatient infections using an administrative data cohort and a chart review cohort, respectively. At the same time this policy was implemented to limit quinolone prescribing, two new quinolone antibiotics were added to the formulary. Using administrative data, we analysed a total of 397,534 unique index visits with regard to overall antibiotic utilization, and through chart review, we analysed 1681 charts of patients with infections of interest to determine the indications for quinolone usage.
Using segmented regression models adjusting for age, sex and physician enrollment in the OSA program, there was no statistically significant change in the monthly rate of all quinolone use (-3.5 (95% CI -5.5, 1.4) prescriptions per 1000 index visits) following implementation of the OSA program (p = 0.74). There was a significant level change in the rate of quinolone antibiotic use for urinary tract infection (-33.6 (95% CI: -23.8, -43.4) prescriptions and upper respiratory tract infection (-16.1 (95%CI: -11.6, -20.6) prescriptions per 1000 index visits. Among quinolone prescriptions identified on chart review, 42.5% and 58.5% were consistent with formulary guidelines before and after the implementation of the OSA program, respectively (p = 0.002). There was no change in hospitalization, mortality or use of physician services after implementation of the OSA program.
Despite the addition of two new quinolone antibiotics to the formulary, we found that there was no change in the use of quinolones after implementation of a new formulary restriction policy for outpatients with common outpatient infections.
公共资助的药品计划通常使用事先授权政策来限制药物处方。为了根据新的处方指南指导具有广泛抗菌活性的一类抗生素(喹诺酮类抗生素)的医生处方,艾伯塔省的省卫生部实施了一项名为可选特殊授权(OSA)计划的新的配方限制机制。我们进行了一项观察性研究,以确定这种新的配方限制政策对抗菌药物处方率的影响以及任何临床后果。
在实施 OSA 计划前后,分别使用行政数据队列和图表审查队列评估常见门诊感染患者的喹诺酮类抗生素使用情况和遵守喹诺酮类药物处方指南的情况。同时,为了限制喹诺酮类药物的处方,该政策还将两种新的喹诺酮类抗生素添加到了配方中。我们使用行政数据总共分析了 397534 例独特的索引就诊,以了解总体抗生素使用情况,并且通过图表审查,我们分析了 1681 例感兴趣感染患者的图表,以确定喹诺酮类药物使用的适应症。
使用分段回归模型调整年龄、性别和医生参与 OSA 计划的情况,在实施 OSA 计划后,喹诺酮类药物的月使用率(每 1000 次索引就诊减少 3.5(95%CI-5.5,1.4)处方)没有统计学意义上的变化(p = 0.74)。喹诺酮类抗生素用于尿路感染(减少 33.6(95%CI:-23.8,-43.4)处方)和上呼吸道感染(减少 16.1(95%CI:-11.6,-20.6)处方)的使用率有显著的水平变化每 1000 次索引就诊。在图表审查中确定的喹诺酮类药物处方中,分别有 42.5%和 58.5%在实施 OSA 计划前后符合配方指南(p = 0.002)。实施 OSA 计划后,住院、死亡率或医生服务的使用没有变化。
尽管在配方中添加了两种新的喹诺酮类抗生素,但我们发现,在为常见门诊感染患者实施新的配方限制政策后,喹诺酮类药物的使用没有变化。