Reproductive Research Division, Pacific Reproductive Center, PRC-Orange County, 10 Post, Irvine, CA 92618, USA.
Reprod Biol Endocrinol. 2012 Aug 30;10:67. doi: 10.1186/1477-7827-10-67.
During in vitro fertilization (IVF), fertility patients are expected to self-administer many injections as part of this treatment. While newer medications have been developed to substantially reduce the number of these injections, such agents are typically much more expensive. Considering these differences in both cost and number of injections, this study compared patient preferences between GnRH-agonist and GnRH-antagonist based protocols in IVF.
Data were collected by voluntary, anonymous questionnaire at first consultation appointment. Patient opinion concerning total number of s.c. injections as a function of non-reimbursed patient cost associated with GnRH-agonist [A] and GnRH-antagonist [B] protocols in IVF was studied.
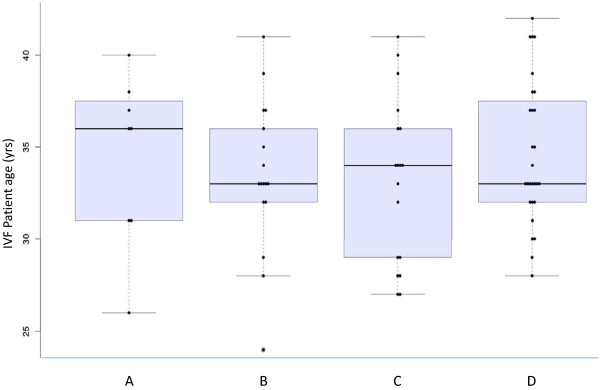
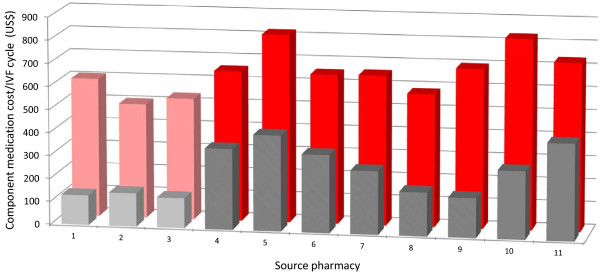
Completed questionnaires (n = 71) revealed a mean +/- SD patient age of 34 +/- 4.1 yrs. Most (83.1%) had no prior IVF experience; 2.8% reported another medical condition requiring self-administration of subcutaneous medication(s). When out-of-pocket cost for [A] and [B] were identical, preference for [B] was registered by 50.7% patients. The tendency to favor protocol [B] was weaker among patients with a health occupation. Estimated patient costs for [A] and [B] were $259.82 +/- 11.75 and $654.55 +/- 106.34, respectively (p < 0.005). Measured patient preference for [B] diminished as the cost difference increased.
This investigation found consistently higher non-reimbursed direct medication costs for GnRH-antagonist IVF vs. GnRH-agonist IVF protocols. A conditional preference to minimize downregulation (using GnRH-antagonist) was noted among some, but not all, IVF patient sub-groups. Compared to IVF patients with a health occupation, the preference for GnRH-antagonist was weaker than for other patients. While reducing total number of injections by using GnRH-antagonist is a desirable goal, it appears this advantage is not perceived equally by all IVF patients and its utility is likely discounted heavily by patients when nonreimbursed medication costs reach a critical level.
在体外受精(IVF)过程中,作为治疗的一部分,生育患者需要自行注射许多针剂。虽然已经开发出更新的药物来大大减少这些注射的数量,但这些药物通常要昂贵得多。考虑到这些在成本和注射次数方面的差异,本研究比较了 GnRH 激动剂和 GnRH 拮抗剂方案在 IVF 中的患者偏好。
通过首次咨询预约时的自愿匿名问卷收集数据。研究了患者对 GnRH 激动剂 [A] 和 GnRH 拮抗剂 [B] 方案中总皮下注射次数的意见,同时考虑了与非报销患者费用相关的非报销患者成本。
完成的问卷(n=71)显示患者平均年龄为 34 +/- 4.1 岁。大多数(83.1%)没有 IVF 治疗经验;2.8%报告了另一种需要自行皮下注射药物的疾病。当 A 和 B 的自付费用相同时,有 50.7%的患者表示更喜欢 B。有健康职业的患者对方案 B 的偏好较弱。A 和 B 的估计患者费用分别为 259.82 美元 +/- 11.75 美元和 654.55 美元 +/- 106.34 美元(p<0.005)。随着成本差异的增加,患者对 B 的偏好有所降低。
本研究发现 GnRH 拮抗剂 IVF 与 GnRH 激动剂 IVF 方案相比,非报销直接药物成本始终较高。一些(但不是所有)IVF 患者亚组注意到了最小化下调(使用 GnRH 拮抗剂)的条件性偏好。与具有健康职业的 IVF 患者相比,对 GnRH 拮抗剂的偏好较弱。虽然使用 GnRH 拮抗剂减少总注射次数是一个理想的目标,但似乎并非所有 IVF 患者都认为这种优势是平等的,而且当非报销药物成本达到临界水平时,患者会强烈地认为其效用会大打折扣。