Department of Medical Research (Lower Myanmar), Yangon, Myanmar.
Malar J. 2012 Sep 4;11:309. doi: 10.1186/1475-2875-11-309.
The use of community volunteers is expected to improve access to accurate diagnosis and timely treatment of malaria, using rapid diagnostic test (RDT) and artemisinin-based combination therapy (ACT). However, empirical data from the field are still limited. The aim of this study was to assess whether training village volunteers on the use of Paracheck-Pf® RDT and ACT (artemether-lumefantrine (AL)) for Plasmodium falciparum and presumptive treatment with chloroquine for Plasmodium vivax had an effect on the coverage of timely diagnosis and treatment and on mortality in malaria-endemic villages without health staff in Myanmar.
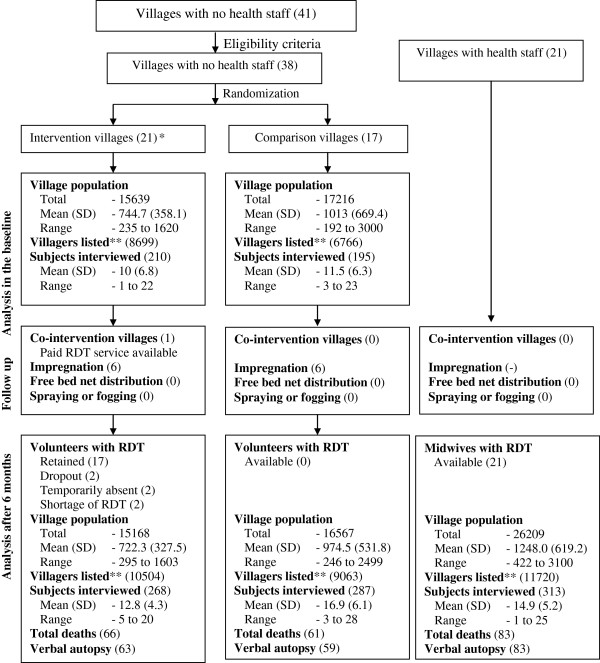
The study was designed as a cluster randomized controlled trial with a cross-sectional survey at baseline, a monthly visit for six months following the intervention (village volunteers trained and equipped with Paracheck-Pf®) and an endline survey at six months follow-up. Survey data were supplemented by the analysis of logbooks and field-based verbal autopsies. Villages with midwives (MW) in post were used as a third comparison group in the endline survey. Intention-to-treat analysis was used.
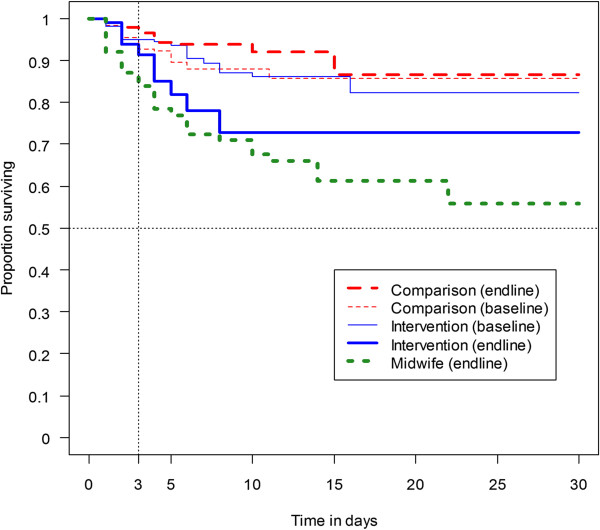
Of 38 villages selected, 21 were randomly assigned to the intervention (two villages failed to participate) and 17 to the comparison group. The two groups had comparable baseline statistics. The blood tests provided by volunteers every month declined over time from 279 tests to 41 but not in MW group in 18 villages (from 326 to 180). In the endline survey, among interviewed subjects (268 intervention, 287 in comparison, 313 in MW), the coverage of RDT was low in all groups (14.9%, SE 2.4% in intervention; 5.7%, SE 1.7% in comparison; 21.4%, SE 2.6% in MW) although the intervention (OR 3.2, 95% CI 1.5-6.7) and MW (OR 5.4, 95% CI 2.6-11.0) were more likely to receive a blood test. Mean (SE) of blood tests after onset of fever in days was delayed (intervention 3.6 (0.3); comparison 4.8 (1.3); MW 3.2 (0.4)). Malaria mortality rates per 100,000 populations in a year were not significantly different (intervention 130 SE 37; comparison 119 SE 34; MW 50 SE 18). None of the dead cases had consulted volunteers.
The results show that implementing volunteer programmes to improve the coverage of accurate and timely diagnosis with RDT and early treatment may be beneficial but the timeliness of detection and sustainability must be improved.
预计使用社区志愿者可提高疟疾的准确诊断和及时治疗的可及性,方法是使用快速诊断检测(RDT)和以青蒿素为基础的联合疗法(ACT)。然而,来自实地的经验数据仍然有限。本研究的目的是评估在没有卫生工作人员的疟疾流行村庄中,对村志愿者进行使用 Paracheck-Pf®RDT 和 ACT(青蒿琥酯-甲氟喹(AL))检测和治疗对及时诊断和治疗的覆盖率以及死亡率的影响。
该研究设计为一项具有横断面调查的群组随机对照试验,在基线时有一次调查,在干预后(培训村志愿者并配备 Paracheck-Pf®)的六个月内每月进行一次调查,在六个月的随访时有一次终线调查。调查数据通过分析日志和实地口头尸检进行补充。在终线调查中,设有助产士(MW)的村庄被用作第三组比较。采用意向治疗分析。
在选择的 38 个村庄中,21 个被随机分配到干预组(两个村庄未能参与),17 个分配到对照组。两组基线统计数据具有可比性。志愿者每月提供的血液检测次数随着时间的推移从 279 次减少到 41 次,但在有 18 个村庄设有 MW 的组中没有减少(从 326 次减少到 180 次)。在终线调查中,在接受访谈的受试者中(干预组 268 人,对照组 287 人,MW 组 313 人),所有组的 RDT 覆盖率都很低(干预组 14.9%,SE 2.4%;对照组 5.7%,SE 1.7%;MW 组 21.4%,SE 2.6%),但干预组(OR 3.2,95%CI 1.5-6.7)和 MW 组(OR 5.4,95%CI 2.6-11.0)更有可能接受血液检测。发热后平均(SE)检测天数延迟(干预组 3.6(0.3);对照组 4.8(1.3);MW 组 3.2(0.4))。每年每 10 万人的疟疾死亡率没有显著差异(干预组 130 SE 37;对照组 119 SE 34;MW 组 50 SE 18)。没有死亡病例咨询过志愿者。
结果表明,实施志愿者计划以提高 RDT 的准确和及时诊断及早期治疗覆盖率可能是有益的,但检测的及时性和可持续性必须得到改善。