National AIDS Control Organization, New Delhi, India.
Lancet. 2010 Nov 20;376(9754):1768-74. doi: 10.1016/S0140-6736(10)60831-8. Epub 2010 Oct 20.
National malaria death rates are difficult to assess because reliably diagnosed malaria is likely to be cured, and deaths in the community from undiagnosed malaria could be misattributed in retrospective enquiries to other febrile causes of death, or vice-versa. We aimed to estimate plausible ranges of malaria mortality in India, the most populous country where the disease remains common.
Full-time non-medical field workers interviewed families or other respondents about each of 122,000 deaths during 2001-03 in 6671 randomly selected areas of India, obtaining a half-page narrative plus answers to specific questions about the severity and course of any fevers. Each field report was sent to two of 130 trained physicians, who independently coded underlying causes, with discrepancies resolved either via anonymous reconciliation or adjudication.
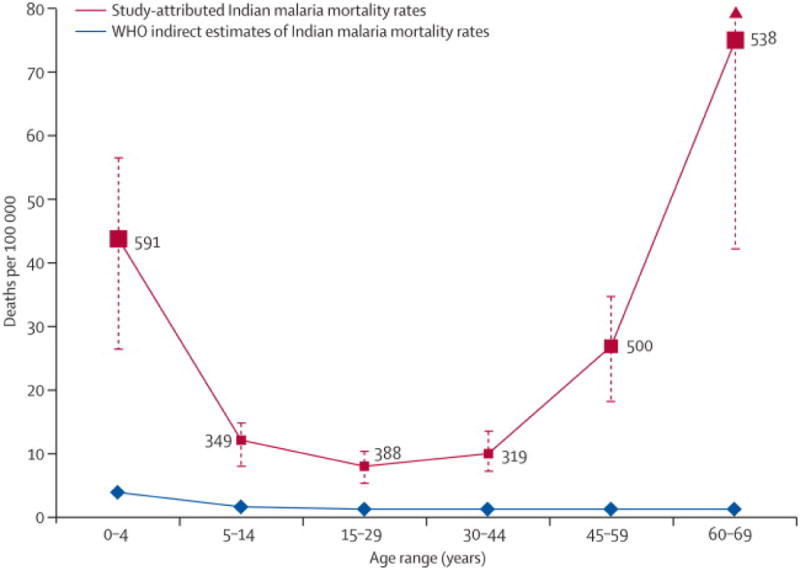
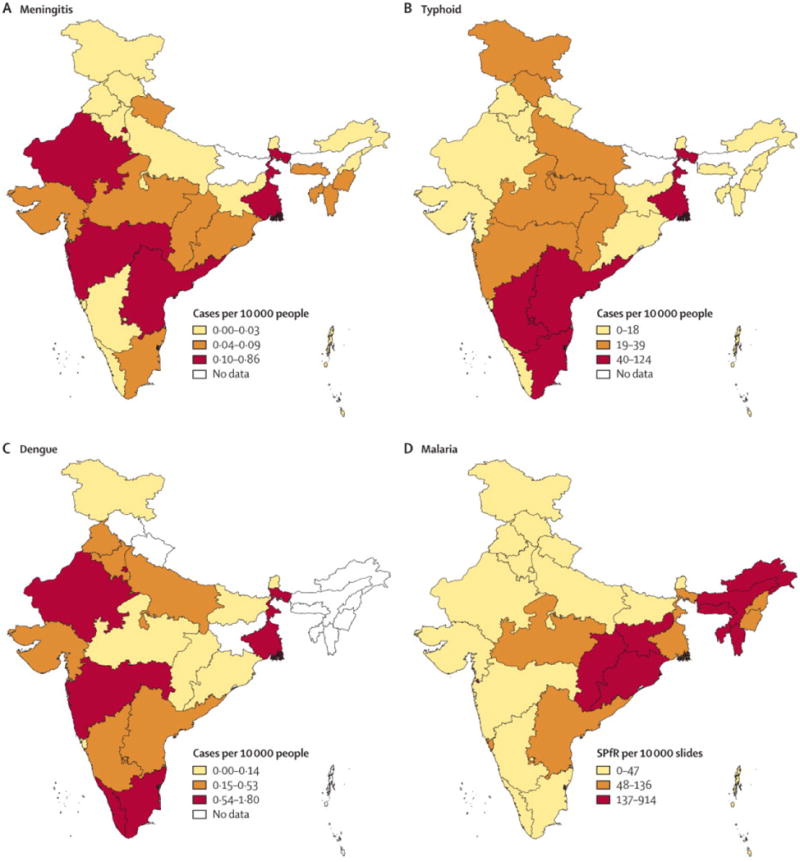
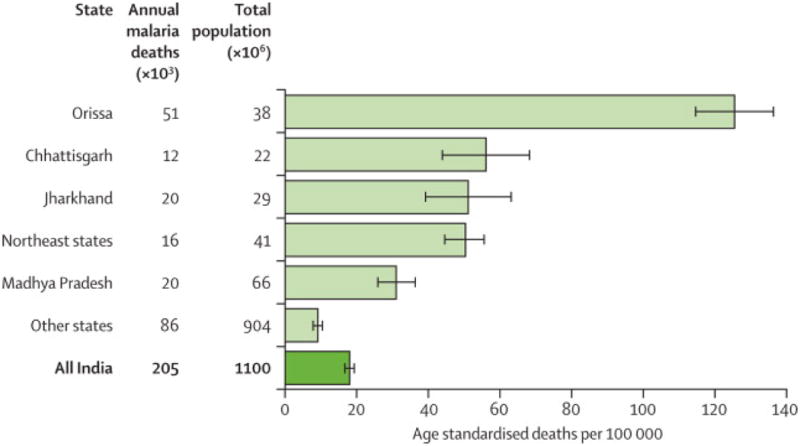
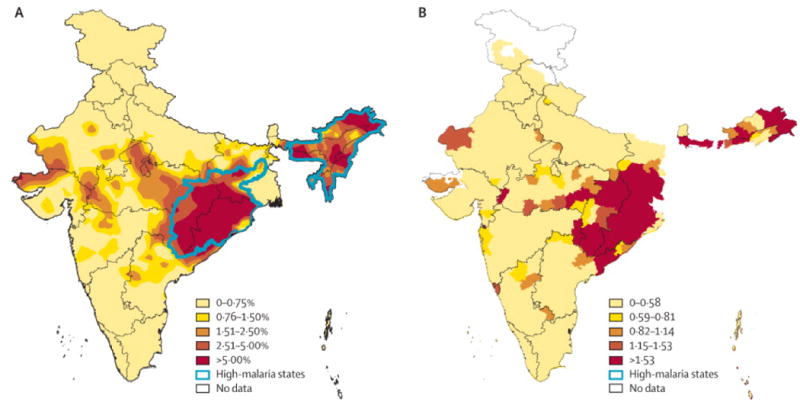
Of all coded deaths at ages 1 month to 70 years, 2681 (3·6%) of 75,342 were attributed to malaria. Of these, 2419 (90%) were in rural areas and 2311 (86%) were not in any health-care facility. Death rates attributed to malaria correlated geographically with local malaria transmission ratesderived independently from the Indian malaria control programme. The adjudicated results show 205,000 malaria deaths per year in India before age 70 years (55,000 in early childhood, 30,000 at ages 5-14 years, 120,000 at ages 15-69 years); 1·8% cumulative probability of death from malaria before age 70 years. Plausible lower and upper bounds (on the basis of only the initial coding) were 125,000-277,000. Malaria accounted for a substantial minority of about 1·3 million unattended rural fever deaths attributed to infectious diseases in people younger than 70 years.
Despite uncertainty as to which unattended febrile deaths are from malaria, even the lower bound greatly exceeds the WHO estimate of only 15,000 malaria deaths per year in India (5000 early childhood, 10 000 thereafter). This low estimate should be reconsidered, as should the low WHO estimate of adult malaria deaths worldwide.
US National Institutes of Health, Canadian Institute of Health Research, Li Ka Shing Knowledge Institute.
由于确诊的疟疾很可能得到治愈,而社区中未确诊的疟疾死亡病例可能在回顾性调查中被错误地归因于其他发热性死因,反之亦然,因此很难评估全国疟疾死亡率。我们旨在评估印度疟疾死亡率的合理范围,印度是人口最多的疟疾流行国家。
全职非医务外勤人员在 2001-2003 年期间,对印度 6671 个随机选定地区的 122000 例死亡进行了调查,获取半页篇幅的叙述,并对任何发热的严重程度和过程回答具体问题。每份实地报告都被发送给 130 名受过培训的医生中的两位,他们独立编码潜在病因,如果存在分歧,则通过匿名和解或裁决来解决。
在 1 个月至 70 岁年龄组的所有编码死亡中,75342 例归因于疟疾的死亡有 2681 例(3.6%)。其中,2419 例(90%)发生在农村地区,2311 例(86%)未在任何医疗机构发生。归因于疟疾的死亡率与从印度疟疾控制规划中独立得出的当地疟疾传播率具有地理相关性。经裁决的结果显示,印度每年 70 岁以下的疟疾死亡人数为 205000 例(55000 例发生在儿童早期,30000 例发生在 5-14 岁,120000 例发生在 15-69 岁);70 岁前死于疟疾的累积概率为 1.8%。仅基于初次编码的合理下限和上限(90%CI)分别为 125000-277000。疟疾在归因于 70 岁以下传染病的约 130 万例农村未就诊发热死亡中占少数(儿童早期 5000 例,以后 10000 例)。尽管对哪些未就诊的发热性死亡是由疟疾引起的存在不确定性,但即使是下限也大大超过了世界卫生组织(WHO)估计的印度每年仅 15000 例疟疾死亡(儿童早期 5000 例,以后 10000 例)。应该重新考虑这一低估计,也应该重新考虑世卫组织对全球成人疟疾死亡人数的低估计。
美国国立卫生研究院、加拿大卫生研究院、李嘉诚知识研究所。