Tsai Naoky, Jeffers Lennox, Cragin Lael, Sorensen Sonja, Su Wenqing, Rosenblatt Lisa, Tang Hong, Hebden Tony, Juday Timothy
John A Burns School of Medicine, University of Hawaii, Honolulu, HI, USA.
Clinicoecon Outcomes Res. 2012;4:227-35. doi: 10.2147/CEOR.S31784. Epub 2012 Aug 23.
Decompensated cirrhosis is a serious clinical complication of chronic hepatitis B (CHB) that places a large economic burden on the US health care system. Although entecavir has been shown to improve health outcomes in a cost-effective manner in mixed populations of CHB patients, the cost-effectiveness of entecavir has not been evaluated in CHB patients with decompensated cirrhosis.
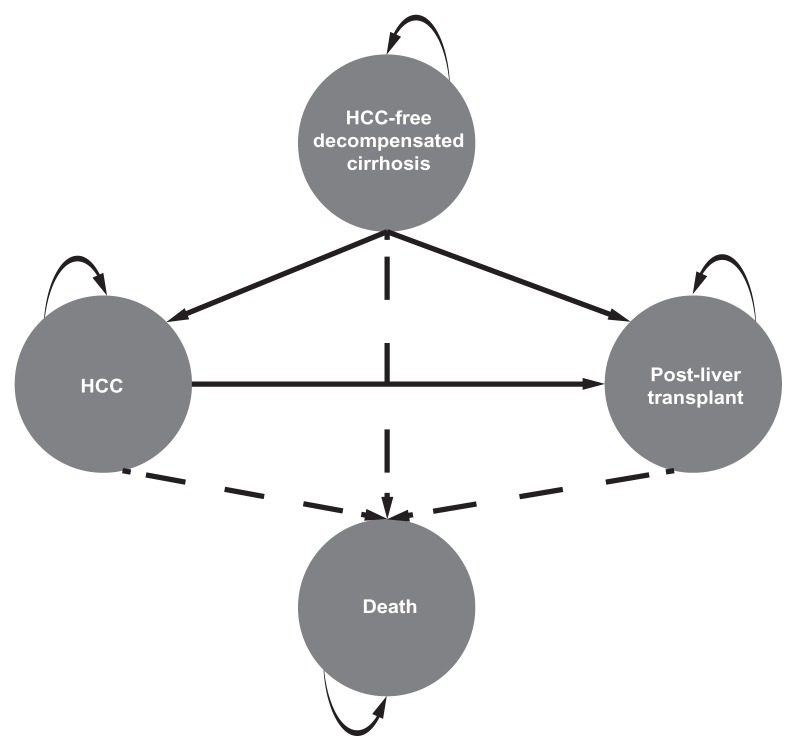
This study assessed the cost-effectiveness of entecavir versus adefovir, from a US payer perspective, in CHB patients with decompensated cirrhosis, using a health-state transition Markov model with four health states: hepatocellular carcinoma (HCC), HCC-free survival, post-liver transplant, and death. The model considered a hypothetical patient population similar to that included in a randomized controlled trial in the target population (ETV-048): predominantly male (74%), Asian (54%), mean age 52 years, hepatic decompensation (Child-Pugh score ≥ seven), hepatitis B e antigen-positive or -negative, treatment-naïve or lamivudine-experienced, and no liver transplant history. Clinical inputs were based on cumulative safety results for ETV-048 and published literature. Costs were obtained from published literature. Costs and outcomes were discounted at 3% per annum.
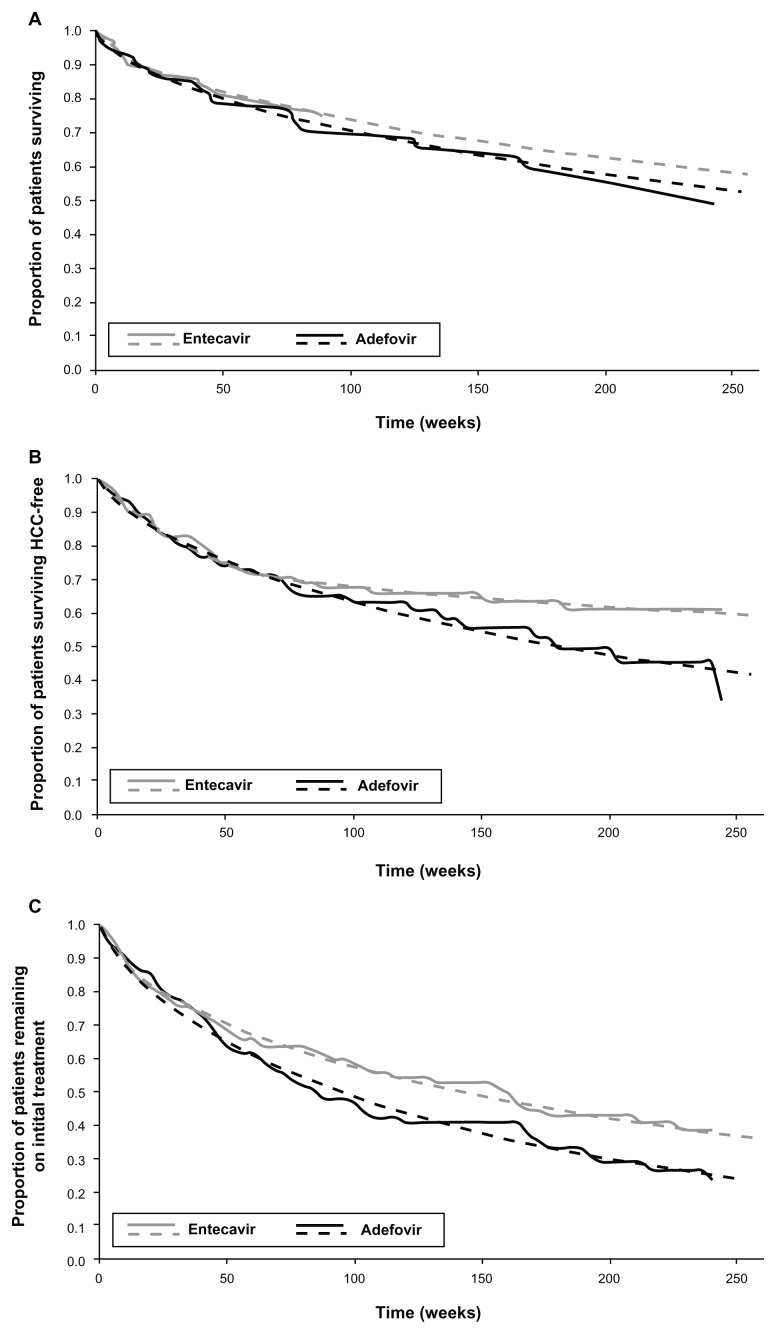
For 1000 patients over a 3-year time horizon, predicted overall survival and HCC-free survival were longer with entecavir than with adefovir (2.35 versus 2.30 years and 2.11 versus 2.03 years, respectively). Predicted total health care costs were $889 lower with entecavir than with adefovir ($91,878 versus $92,768). For incremental cost/life-year gained and incremental cost/HCC-free-year gained, entecavir was less costly and more effective than adefovir. Sensitivity analyses found the results to be robust to plausible variations in health-state costs and discount rate.
This analysis suggests that entecavir improves survival outcomes in a cost-saving manner compared with adefovir in CHB patients with hepatic decompensation.
失代偿期肝硬化是慢性乙型肝炎(CHB)的一种严重临床并发症,给美国医疗保健系统带来了巨大的经济负担。尽管在CHB患者的混合人群中,恩替卡韦已被证明能以具有成本效益的方式改善健康结局,但恩替卡韦在失代偿期肝硬化CHB患者中的成本效益尚未得到评估。
本研究从美国支付方的角度,使用具有四个健康状态的健康状态转换马尔可夫模型,评估恩替卡韦与阿德福韦在失代偿期肝硬化CHB患者中的成本效益,这四个健康状态为:肝细胞癌(HCC)、无HCC生存、肝移植后和死亡。该模型考虑了一个假设的患者群体,类似于目标人群(ETV-048)的一项随机对照试验中纳入的群体:主要为男性(74%)、亚洲人(54%),平均年龄52岁,肝失代偿(Child-Pugh评分≥7),乙肝e抗原阳性或阴性,初治或有拉米夫定治疗史,且无肝移植史。临床输入基于ETV-048的累积安全性结果和已发表的文献。成本来自已发表的文献。成本和结局按每年3%进行贴现。
在3年的时间范围内,对于1000名患者,恩替卡韦组预测的总生存期和无HCC生存期比阿德福韦组长(分别为2.35年对2.30年和2.11年对2.03年)。恩替卡韦组预测的总医疗成本比阿德福韦组低889美元(91,878美元对92,768美元)。对于增量成本/生命年增益和增量成本/无HCC年增益,恩替卡韦比阿德福韦成本更低且更有效。敏感性分析发现,结果对于健康状态成本和贴现率的合理变化具有稳健性。
该分析表明,在肝失代偿的CHB患者中,与阿德福韦相比,恩替卡韦能以节省成本的方式改善生存结局。