University of Missouri Medical Center, Columbia, MO, USA.
Pediatr Rheumatol Online J. 2012 Sep 20;10(1):34. doi: 10.1186/1546-0096-10-34.
We tested the hypothesis that the course and outcome of juvenile dermatomyositis (JDM) in children seen at one center with the JDM disease onset at or below three years of age is different from that in the children with disease onset at greater than three years of age.
Institutional Review Board approval was obtained to retrospectively review the charts of 78 patients from age 0-18 years with JDM seen in the pediatric rheumatology clinic at Nationwide Children's Hospital in Columbus, Ohio over the past 23 years from January 1988. The diagnosis was made by the treating pediatric rheumatologist. Not all the patients met the Bohan and Peter criteria, as muscle biopsy and EMG were not always performed and we utilized a modified JDM criteria. The data regarding disease course and outcome were collected as of the last clinic follow-up or to July 1, 2010. We used the Wilcoxon Two-Sample test to compare numerical variables between two age groups, and used logistic regression to compare categorical variables between two age groups in SAS 9.1.3. Minitab-16 was used to calculate various mean, median, modes, standard deviations and range. For survival analysis, we used Kaplan-Meier method with log-rank test.
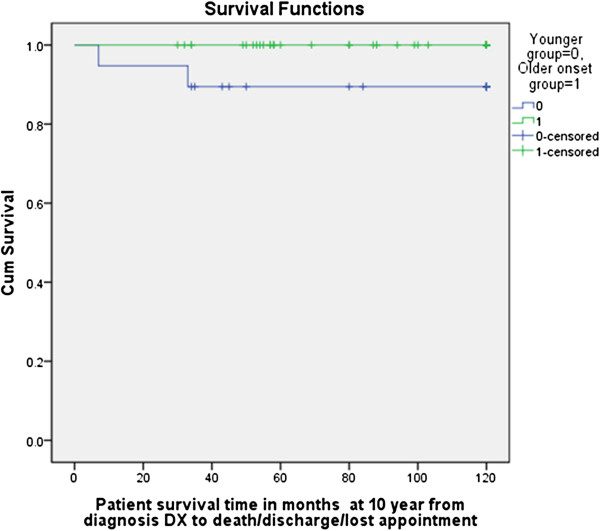
The mean age of onset in the two groups at Nationwide Children's Hospital was 27 months and 91 months. The mean times between onset of symptoms to diagnosis in the younger and older age groups was 5.6 months and 4.5 months, respectively, not a statistically significant difference. The younger onset group had more females (p=0.05) and their disease onset occurred less frequently during the typical winter-spring seasons (p=0.031). The younger onset group was more likely to have a preceding fever (p=0.029) and family history of autoimmune diseases (p=0.012). The younger onset group was less likely to have heliotrope rash (p=0.04), Gottron's sign (p=0.049), capillary loop abnormalities (p=0.010), or elevations in creatine kinase (CK, p=0.022), aspartate aminotransferase (AST, p=0.021) or aldolase (p=0.035). The younger onset group was treated less often with pulse methylprednisolone at diagnosis (p=0.043) and less often with hydroxychloroquine (p=0.035). There were no differences between the two groups regarding initial oral steroid dose (p=0.8017), number of patients who received methotrexate at diagnosis (p=0.709), and the number who ever received other immunosuppressants (p=0.323). The mean and maximum duration (mean duration 24.3 months vs. 35.2 months, maximum duration 51 vs. 124 months in younger and older onset group respectively) of methotrexate therapy, and the mean and maximum duration of oral steroid therapy (Mean duration 16.8 months vs. 33.3 months, maximum duration 50 vs. 151 months in younger and older onset group respectively), was shorter in the younger group. The younger onset patients were less likely to have active disease at 5 years (9% vs. 35.7%, p=0.015) and 10 years post-diagnosis (9% vs. 45.1%, p=0.011, Table 7). The younger patients were less likely to have osteonecrosis (p=0.023). Two disease-related deaths occurred in the younger group, none in the older group. The results of the survival analysis showed that the difference between the age groups was statistically significant (p < 0.012). The sex and race were not significant (p> 0.26 and p>0.95, respectively).
There were significant differences between JDM patients with disease onset at or below age three years at our center, compared to their older counterparts. Younger patients in our cohort had fewer typical findings at diagnosis and a milder disease course without needing as long a duration of corticosteroids and immunosuppression. Patients with a younger onset had a higher mortality rate but mortalities were unusual and numbers small. The younger group had a similar complication rate compared to the older onset patients, except for osteonecrosis which was higher in the older onset group. These findings differ from the previous reports that a younger age of onset in JDM is often associated with a more severe disease, as results at our center suggest that children with younger onset JDM appear to be atypical but may do well compared to the older JDM patients.
我们检验了这样一个假说,即我们中心发病年龄在 3 岁及以下的儿童与发病年龄大于 3 岁的儿童相比,皮肌炎(JDM)的病程和结局有所不同。
我们获得机构审查委员会的批准,回顾了过去 23 年来俄亥俄州哥伦布市全国儿童医院儿科风湿病门诊就诊的 78 名 JDM 患儿的病历,这些患儿的年龄在 0-18 岁之间,发病年龄在 1988 年 1 月之前。诊断由治疗小儿风湿病的医生做出。并非所有患者都符合 Bohan 和 Peter 标准,因为并非总是进行肌肉活检和肌电图检查,并且我们采用了改良的 JDM 标准。关于疾病过程和结局的数据是在最后一次门诊随访或 2010 年 7 月 1 日收集的。我们使用 Wilcoxon 两样本检验比较了两个年龄组的数值变量,使用逻辑回归比较了两个年龄组的分类变量,SAS 9.1.3 用于 Minitab-16 计算各种均值、中位数、众数、标准差和范围。对于生存分析,我们使用 Kaplan-Meier 方法和对数秩检验。
全国儿童医院两个年龄组的平均发病年龄分别为 27 个月和 91 个月。在较小年龄组和较大年龄组中,症状出现到诊断的平均时间分别为 5.6 个月和 4.5 个月,差异无统计学意义。发病年龄较小的患儿女性更多(p=0.05),发病季节不太常见于典型的冬春季节(p=0.031)。发病年龄较小的患儿更可能出现前驱发热(p=0.029)和自身免疫性疾病家族史(p=0.012)。发病年龄较小的患儿发生眶周水肿(p=0.04)、Gottron 征(p=0.049)、毛细血管环异常(p=0.010)、肌酸激酶(CK,p=0.022)、天门冬氨酸氨基转移酶(AST,p=0.021)或醛缩酶(p=0.035)升高的可能性较低。发病年龄较小的患儿在诊断时较少接受脉冲甲基强的松龙治疗(p=0.043),较少接受羟氯喹治疗(p=0.035)。两组之间在初始口服类固醇剂量(p=0.8017)、诊断时接受甲氨蝶呤的患者人数(p=0.709)以及接受其他免疫抑制剂的患者人数(p=0.323)方面无差异。发病年龄较小的患儿接受甲氨蝶呤治疗的平均和最长持续时间(平均持续时间 24.3 个月 vs. 35.2 个月,最长持续时间 51 个月 vs. 124 个月)以及口服类固醇治疗的平均和最长持续时间(平均持续时间 16.8 个月 vs. 33.3 个月,最长持续时间 50 个月 vs. 151 个月)均较短。发病年龄较小的患儿在诊断后 5 年(9% vs. 35.7%,p=0.015)和 10 年(9% vs. 45.1%,p=0.011)时疾病活动的可能性较低,见表 7。发病年龄较小的患儿发生骨坏死的可能性较低(p=0.023)。两个年龄组中均有 2 例与疾病相关的死亡,发病年龄较小组 1 例,发病年龄较大组无死亡。生存分析结果表明,两组之间的差异具有统计学意义(p<0.012)。性别和种族无显著差异(p>0.26 和 p>0.95)。
与我们中心发病年龄大于 3 岁的患者相比,发病年龄在 3 岁及以下的皮肌炎患儿存在显著差异。我们队列中的年幼患者在诊断时的典型表现较少,疾病过程较轻,无需长期使用皮质类固醇和免疫抑制剂。发病年龄较小的患者死亡率较高,但死亡率不常见,且数量较少。与发病年龄较大的患者相比,发病年龄较小的患者的并发症发生率相似,除了骨坏死的发生率较高,而骨坏死在发病年龄较大的患者中更为常见。这些发现与之前的报告不同,即皮肌炎的发病年龄较小通常与更严重的疾病有关,而我们中心的结果表明,发病年龄较小的皮肌炎患儿似乎不典型,但与发病年龄较大的皮肌炎患者相比可能预后较好。